Spondylitis ankylosans






























Ankylosing spondylitis (less commonly known as Bechterew disease or Marie Strümpell disease) is a seronegative spondyloarthropathy, which results in fusion (ankylosis) of the spine and sacroiliac (SI) joints, although involvement is also seen in large and small joints.
Epidemiology
Traditionally it was thought there was a male predilection of 3:1 or more, however the gender predilection of the disease is a matter of recent debate and research (females may be under-diagnosed). According to some research men tend towards more severe disease . The disease usually manifests in young adults, with the first symptoms becoming evident in the third decade, although up to 18% of cases manifest in the second decade.
Associations
- anterior uveitis (25-40%)
- psoriasis
- inflammatory bowel disease: ulcerative colitis/Crohn disease
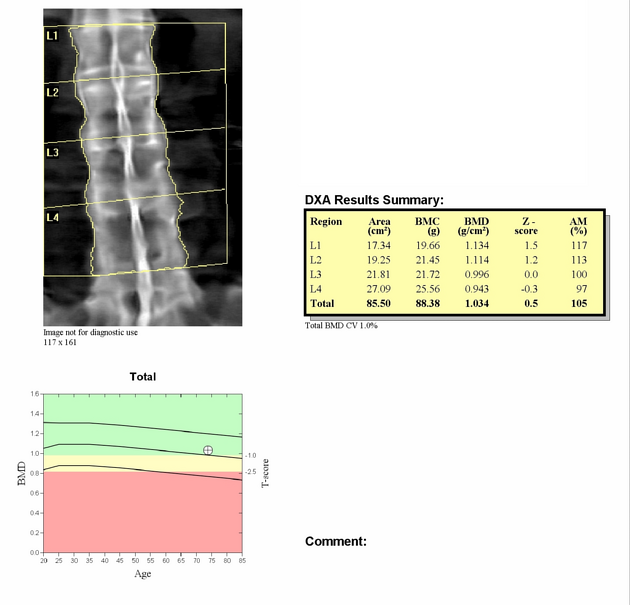
- osteopenia
- cardiovascular disease
- apical/upper lobe predominant interstitial lung disease with small cystic spaces (in ~1% of patients)
- aortic valve disease / aortitis
- secondary amyloidosis (rare)
- cauda equina syndrome (rare)
Pathology
Genetics
Patients are rheumatoid factor (RF) negative, hence seronegative. HLA B27 is the gene with the strongest association. Other possibly contributing genes include ERAP-1, IL23R and TNF-associated genes . Although approximately 90% of Caucasian individuals with ankylosing spondylitis have the HLA-B27 gene, it is important to note this gene is present in 8-9% of people of Northern European ancestry . Overall, ~5% of people positive for HLA-B27 develop ankylosing spondylitis.
Radiographic features
The axial skeleton is predominantly affected, although in ~20% of cases the peripheral joints are also involved.
Plain radiograph
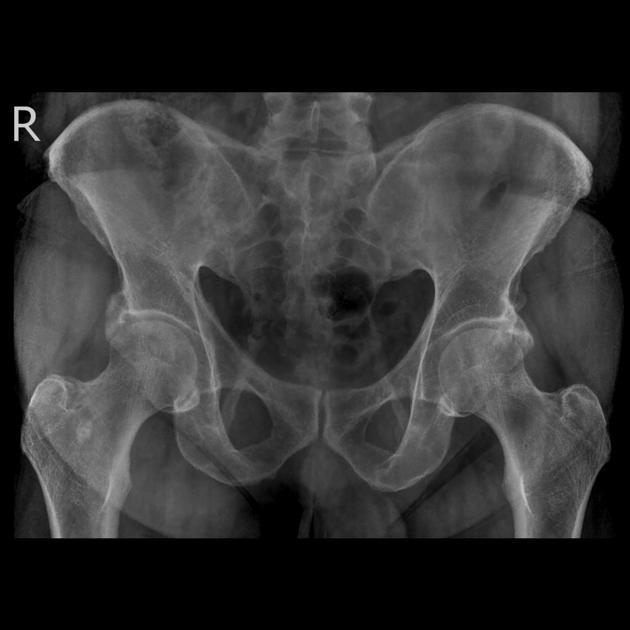
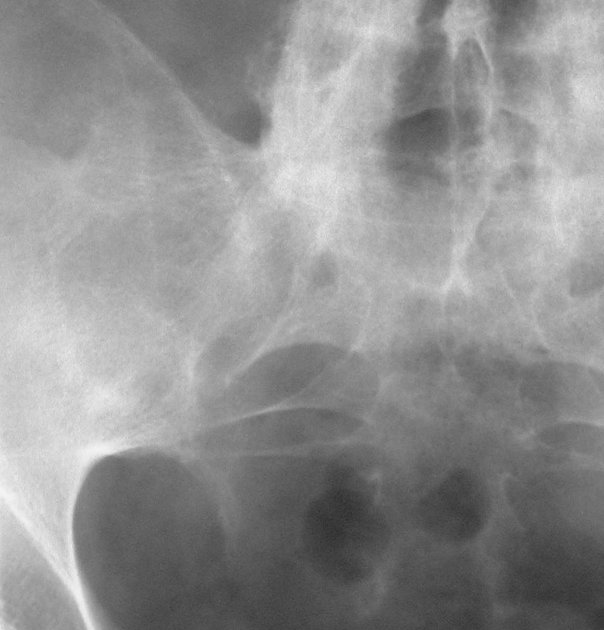
Sacroiliac joints
- sacroiliitis is usually the first manifestation and is symmetrical and bilateral
- the sacroiliac joints first widen before they narrow
- subchondral erosions, sclerosis, and proliferation on the iliac side of the SI joints
- at end-stage, the SI joint may be seen as a thin line or not visible
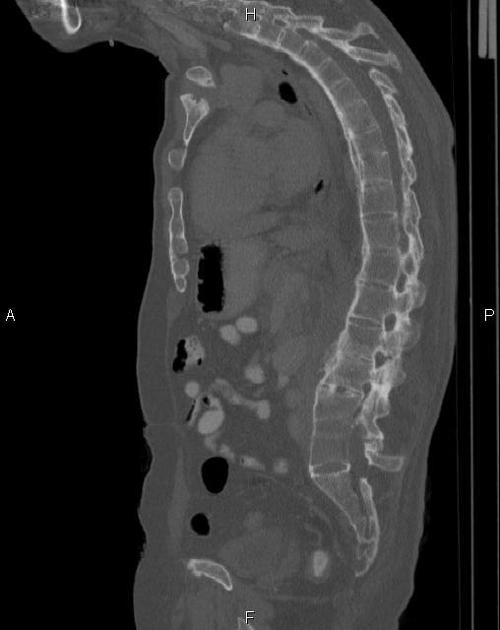
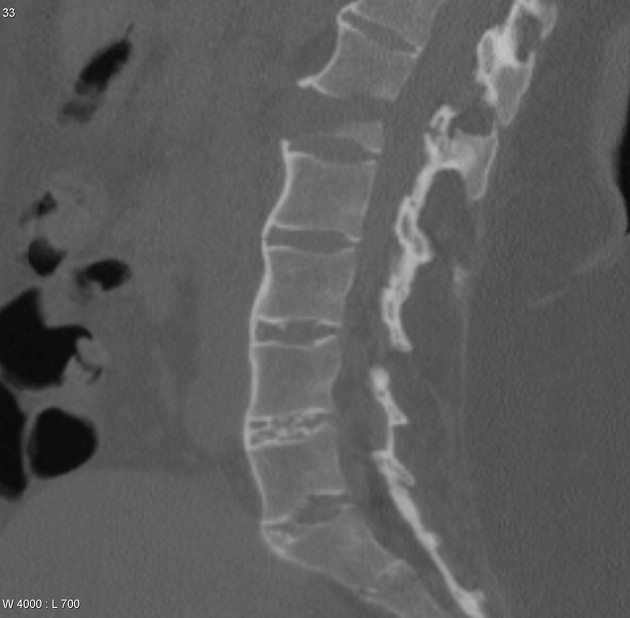
Spine
- early spondylitis is characterized by small erosions at the corners of vertebral bodies with reactive sclerosis: Romanus lesions of the spine (shiny corner sign)
- vertebral body squaring
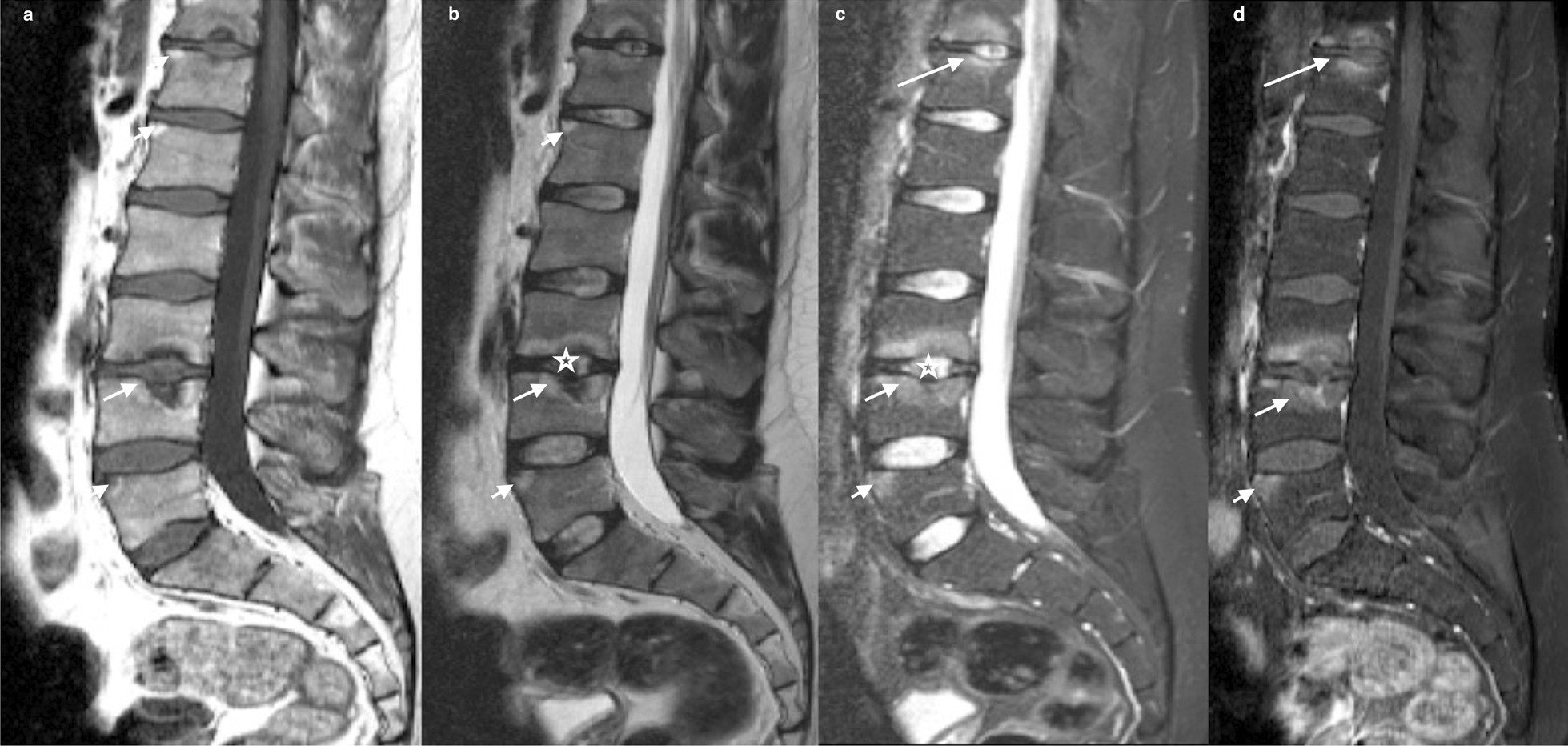
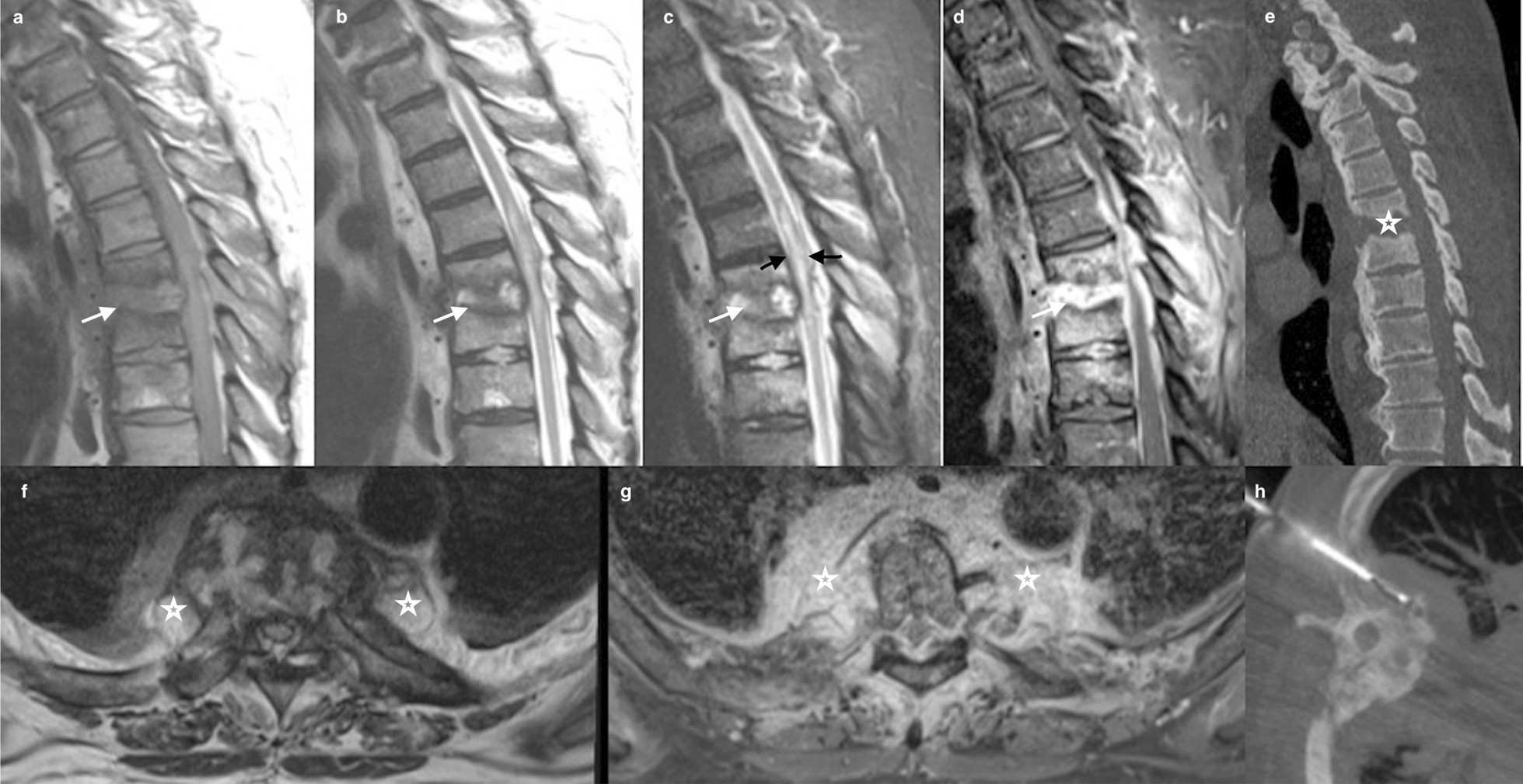
- noninfectious spondylodiskitis: Andersson lesion
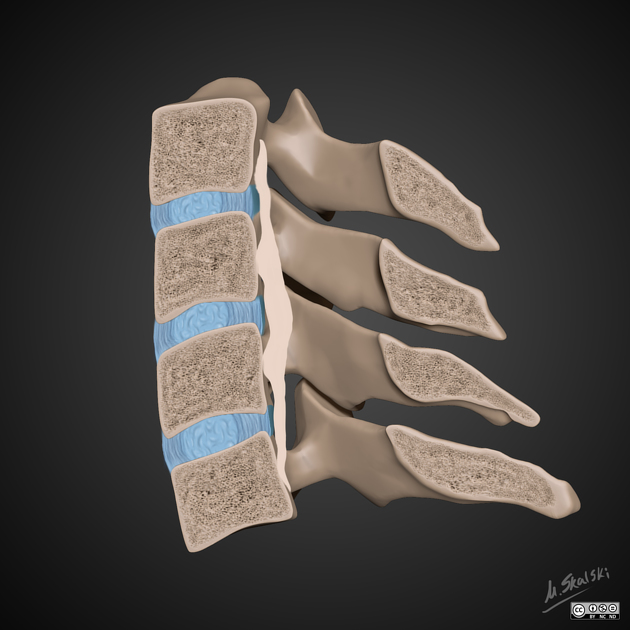
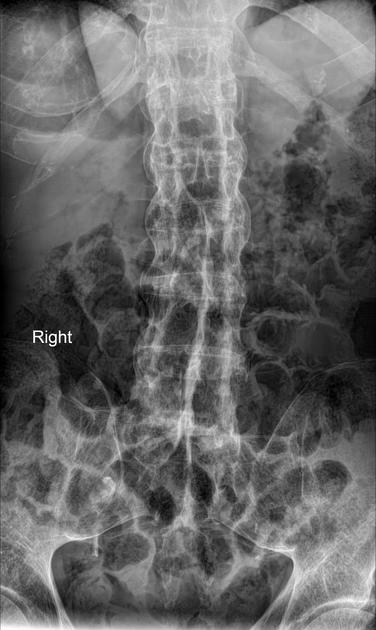
- diffuse syndesmophytic ankylosis can give a "bamboo spine" appearance
- syndesmophytes are classically described as paravertebral ossification running parallel to the spine
- linear ossification along the central spine; representing interspinous ligament ossification can give a "dagger spine" appearance on frontal radiographs;
- ossification of spinal ligaments, joints and discs (with fatty marrow within the ossified disc, best seen on MRI)
- apophyseal and costovertebral arthritis and ankylosis
- enthesophyte formation from enthesopathy
- pseudoarthroses may form at fracture sites
- dural ectasia
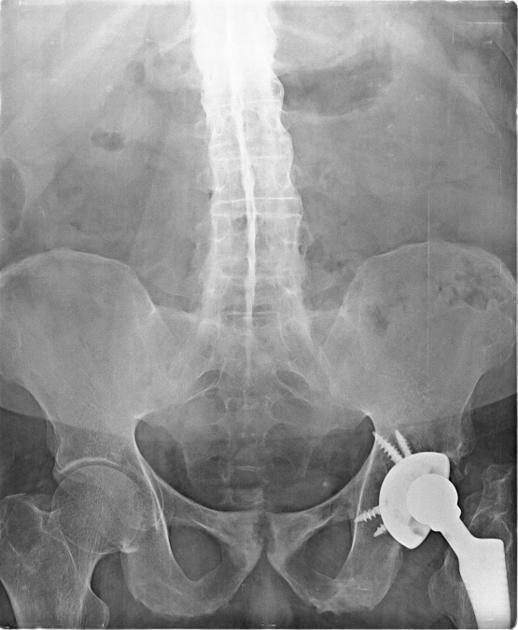
Hips
Hip involvement is generally bilateral and symmetric, with uniform joint space narrowing, axial migration of the femoral head sometimes reaching a state of protrusio acetabuli, and a collar of osteophytes at the femoral head-neck junction.
Pelvis
There can be bridging or fusion of the pubic symphysis.
Knees
Knees demonstrate uniform joint space narrowing with bony proliferation.
Hands
Hands are generally involved asymmetrically, with smaller, shallower erosions and marginal periostitis.
Shoulders
- Shoulder joint involvement is not uncommon and demonstrates a large erosion of the anterolateral aspect of the humeral head, producing a 'hatchet' deformity.
- Marrow edema of acromion process, at the site of origin of deltoid muscle has been described as a very specific sign of the disease.
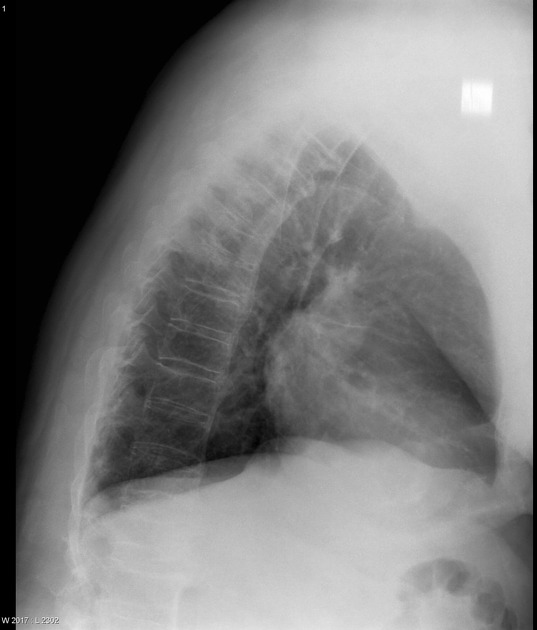
Chest
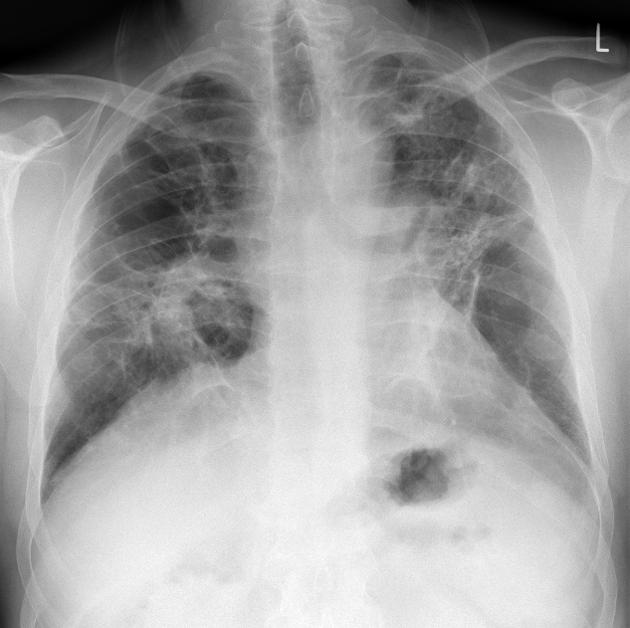
Radiographs of the lungs may demonstrate progressive fibrosis and bullous changes at the apices. These lesions may resemble tuberculosis infection and bullae may become infected.
See: thoracic manifestations of ankylosing spondylitis
Cardiac
Plain radiograph may be normal, or may reveal cardiomegaly.
See: cardiovascular manifestations of ankylosing spondylitis
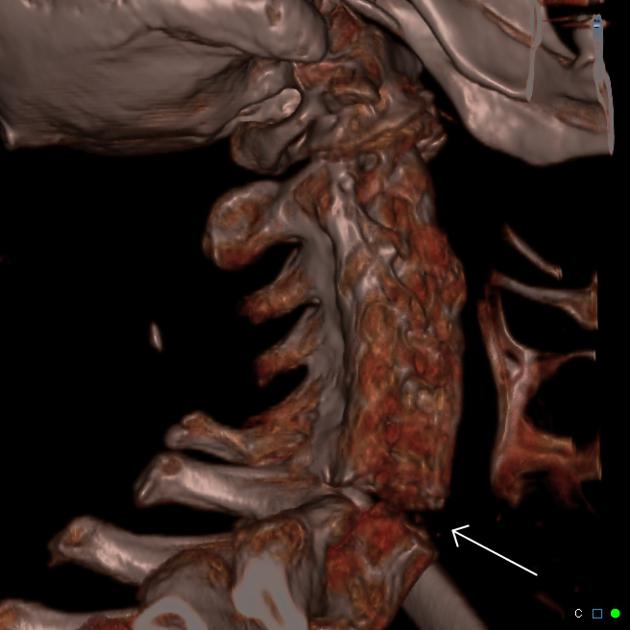
CT
- may be useful in selected patients with normal or equivocal findings on sacroiliac joint radiographs
- chronic structural changes such as joint erosions, subchondral sclerosis, and bony ankylosis are better visualized on CT than on MRI or radiographs
- some normal variants of the SI joints may mimic features of sacroiliitis
- supplements scintigraphy in evaluating areas of increased uptake
- superior to radiographs and MRI in demonstrating injuries
- imaging modality of choice in patients with advanced ankylosing spondylitis in whom there is suspicion of cervical spine fracture
- sagittal reformats should be obtained as axial images poorly assess the transverse fracture plane
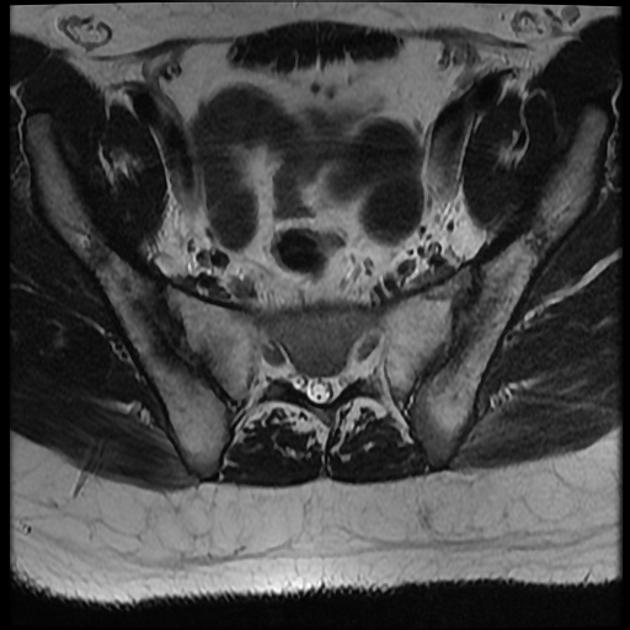
MRI
- may have a role in early diagnosis of sacroiliitis; MRI is more sensitive than CT or plain radiography in detecting inflammatory changes (which precede structural changes) such as bone marrow edema (best demonstrated on STIR sequences), synovitis and capsulitis (on gadolinium enhanced T1 weighted sequences)
- synovial enhancement on MR correlates with disease activity measured by inflammatory mediators
- enhancement of the interspinous ligaments is indicative of enthesitis
- increased T2 signal correlates with edema or vascularized fibrous tissue
- superior to CT in the detection of cartilage inflammation and destruction
- useful in following treatment results in patients with active ankylosing spondylitis
Bone scintigraphy
- maybe helpful in selected patients with normal or equivocal findings on sacroiliac joint radiographs
- qualitative assessment of accumulation of radionuclide in the SI joints may be difficult due to normal uptake in this location; thus, quantitative analysis may be more useful
- ratios of SI joint to sacral uptake of 1.3:1 or higher is abnormal
Treatment and prognosis
First-line therapy is primarily focused on NSAIDs and non-pharmacological measures including education, exercise, physiotherapy and group-therapy. Together, these treatments can lead to substantial clinical improvement in 70-80% of patients. Local steroid injection and DMARDs (sulfasalazine and methotrexate) can also help with peripheral manifestations. Second-line therapy includes TNF-alpha blockers (etanercept, infliximab, adalimumab, certolizumab, golimumab) and IL17 inhibitors (secukinumab) . Whether TNF-alpha blockers can inhibit radiographic disease progression has been the subject of some debate and continues to be investigated .
Complications
- fracture
- diffuse paraspinal ossification and inflammatory osteitis creates a fused, brittle spine, susceptible to fracture, even with minor trauma
- more common at the thoracolumbar and cervicothoracic junctions
- recognition of minimally displaced fractures is difficult due to osteopenia and deformity, and it is important to specifically search for disc space widening and discontinuity of the ossified paraspinal ligaments
- also known as "chalk stick" or "carrot stick fractures"
- Andersson lesion: inflammatory spondylodiskitis that occurs in association with ankylosing spondylitis and results in a disc pseudarthrosis
- rare neurological complications include transverse myelitis and/or cauda equina syndrome
Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)
It is a subjective assessment by the patient on a scale of 1- 10 (least to most severe) in the following six parameters
Differential diagnosis
- general spine: enteropathic arthritis
- cervical spine: juvenile rheumatoid arthritis
- diffuse idiopathic skeletal hyperostosis
Siehe auch:
- Romanus-Läsion
- Osteitis condensans ilii
- Blockwirbel Halswirbelsäule
- Bambusstabwirbelsäule
- Wirbelsäulenfrakturen bei Morbus Bechterew
- Spondylodiscitis
- Diffuse idiopathische Skeletthyperostose
- Andersson lesion
- costovertebrale Ankylose
- dagger sign
- seronegative Spondyloarthropathie
und weiter:
- Ankylose
- Läsionen der Rippen
- Andersson-Läsion
- Protrusio acetabuli
- Aortitis
- Ileitis terminalis
- Ossifikation Ligamentum longitudinale posterius
- Syndesmophyten
- Amyloidose
- Sakroiliitis
- Kastenwirbel
- Aneurysma Aorta ascendens
- chronic periaortitis
- Parenchymband
- Interstitielle Lungenerkrankung
- Duraektasie
- interstitial pneumonia
- Enthesitis
- Diskusverkalkungen
- Blockwirbelbildung bei Morbus Bechterew
- Spondylitis
- vertebral body squaring
- Fersensporn
- thoracic aortic dilatation
- Iliosakralgelenksarthrose
- ISG-Sklerose
- Rheuma Differentialdiagnose
- temporomandibular joint inflammation
- pulmonary upper zone involvement (mnemonic)
- verkalkte Bänder
- respiratory failure
- spondyloarthropathy
- Erweiterung des interpedunculären Abstands
- infectious spondylitis
- upper lobe pulmonary fibrosis (mnemonic)
- pseudoarthrosis of the spine in ankylosing spondylitis
- sacroiliac joint ankylosis
- activated spondylarthritis
- plantarer Fersensporn
- ankylosing spondylitis of the cervical spine
- Plantarfasziitis
- low endplate signal on T1
- radiologisches muskuloskelettales Curriculum
- manubriosternale Ankylose
- ankylosing spondylitis of the lumbar spine
- Differenzialdiagnosen bei Tracheomalazie
- cauda equina syndrome as a complication of ankylosing spondylitis
- Chalk-Stick-Fraktur
- septic arthritis in ankylosing spondylitis


 Assoziationen und Differentialdiagnosen zu Morbus Bechterew:
Assoziationen und Differentialdiagnosen zu Morbus Bechterew:





