Rezidiv bei Nierenzellkarzinom in der Vena cava inferior

Recurrent
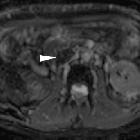
malignant caval thrombosis: value of diffusion-weighted MRI. Portal venous phase acquisition confirmed right nephrectomy without local tumour recurrence in the surgical bed, normal left kidney with opacified renal vein (arrow), near-complete filling defect in the inferior vena cava (arrowheads).
Isolated
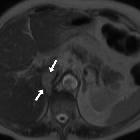
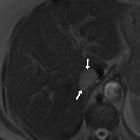
intracaval recurrence of resected renal carcinoma. Unenhanced T2- (a-d) and T1-weighted (e) images showed tumour thrombosis in the intrahepatic vena cava (arrows) and normal flow-void signal at the hepatic vein confluence (arrowheads).

Isolated
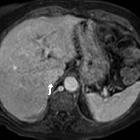
intracaval recurrence of resected renal carcinoma. Dynamic contrast-enhanced MRI acquisition showed strong enhancement in the tumour thrombus (arrows) in the arterial phase (f), portal phase (g) and delayed phase (h).

Isolated
intracaval recurrence of resected renal carcinoma. Dynamic contrast-enhanced MRI acquisition showed strong enhancement in the tumour thrombus (arrows) in the arterial phase (f), portal phase (g) and delayed phase (h).

Isolated
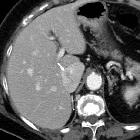
intracaval recurrence of resected renal carcinoma. Follow-up contrast-enhanced CT after sunitinib therapy showed dramatic size decrease of tumor thrombosis (a, b) at six months (arrows) and only a small filling defect (c, d) at three years (arrows).

Isolated
intracaval recurrence of resected renal carcinoma. Follow-up contrast-enhanced CT after sunitinib therapy showed dramatic size decrease of tumor thrombosis (a,b ) at six months (arrows) and only a small filling defect (c, d) at three years (arrows).

Isolated
intracaval recurrence of resected renal carcinoma. Follow-up contrast-enhanced CT after sunitinib therapy showed dramatic size decrease of tumor thrombosis (a, b) at six months (arrows) and only a small filling defect (c, d) at three years (arrows).
Isolated
intracaval recurrence of resected renal carcinoma. Follow-up contrast-enhanced CT after sunitinib therapy showed dramatic size decrease of tumor thrombosis (a, b) at six months (arrows) and only a small filling defect (c, d) at three years (arrows).
Isolated
intracaval recurrence of resected renal carcinoma. Unenhanced T2- (a-d) and T1-weighted (e) images showed tumour thrombosis in the intrahepatic vena cava (arrows) and normal flow-void signal at the hepatic vein confluence (arrowheads).
Isolated
intracaval recurrence of resected renal carcinoma. Unenhanced T2- (a-d) and T1-weighted (e) images showed tumour thrombosis in the intrahepatic vena cava (arrows) and normal flow-void signal at the hepatic vein confluence (arrowheads).
Isolated
intracaval recurrence of resected renal carcinoma. Unenhanced T2- (a-d) and T1-weighted (e) images showed tumour thrombosis in the intrahepatic vena cava (arrows) and normal flow-void signal at the hepatic vein confluence (arrowheads).

Isolated
intracaval recurrence of resected renal carcinoma. Unenhanced T2- (a-d) and T1-weighted (e) images showed tumour thrombosis in the intrahepatic vena cava (arrows) and normal flow-void signal at the hepatic vein confluence (arrowheads).

Recurrent
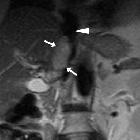
malignant caval thrombosis: value of diffusion-weighted MRI. Coronal image confirmed sizeable filling defect (arrowheads) with 3.5 cm craniocaudal diameter causing minimal dilatation of the inferior vena cava; note unopacified (+) distal lumen due to acquisition before venous return from the extremities.


Isolated
intracaval recurrence of resected renal carcinoma. The left renal vein (thin arrows) and infrahepatic vena cava (thick arrows) were homogeneously opacified, without signs of thrombosis. The left kidney showed normal size, parenchymal opacification and contrast excretion, without hydronephrosis.

Isolated
intracaval recurrence of resected renal carcinoma. Delayed images (c...e): the sizeable, faint filling defect (arrows) in the intrahepatic inferior vena cava persisted in the delayed acquisition. Note metallic clips from previous radical nephrectomy without local recurrence or adenopathies.

Isolated
intracaval recurrence of resected renal carcinoma. Portal venous phase images (a, b): sizeable, faint filling defect (arrows) in the intrahepatic inferior vena cava. Note metallic clips from previous radical nephrectomy without local recurrence in the surgical bed or adenopathies.

Isolated
intracaval recurrence of resected renal carcinoma. Portal venous phase images (a, b): sizeable, faint filling defect (arrows) in the intrahepatic inferior vena cava.

Recurrent
malignant caval thrombosis: value of diffusion-weighted MRI. Diffusion-weighted (b=800) images (f,g) showed marked hyperintense signal of the IVC thrombus (arrowheads) with corresponding hypointensity on apparent diffusion coefficient (ADC) maps (h,i). Mean measured ADC value 0.85x10-3 mm2/s.
Recurrent
malignant caval thrombosis: value of diffusion-weighted MRI. Diffusion-weighted (b=800) images (f,g) showed marked hyperintense signal of the IVC thrombus (arrowheads) with corresponding hypointensity on apparent diffusion coefficient (ADC) maps (h,i). Mean measured ADC value 0.85x10-3 mm2/s.

Recurrent
malignant caval thrombosis: value of diffusion-weighted MRI. Diffusion-weighted (b=800) images (f,g) showed marked hyperintense signal of the IVC thrombus (arrowheads) with corresponding hypointensity on apparent diffusion coefficient (ADC) maps (h,i). Mean measured ADC value 0.85x10-3 mm2/s.

Recurrent
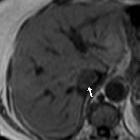
malignant caval thrombosis: value of diffusion-weighted MRI. On fat-suppressed T1-weighted images the thrombus (arrowheads) showed low-to-intermediate signal intensity, with speckled hypersignal foci (thin arrows).
Isolated
intracaval recurrence of resected renal carcinoma. Dynamic contrast-enhanced MRI acquisition showed strong enhancement in the tumour thrombus (arrows) in the arterial phase (f), portal phase (g) and delayed phase (h).
Rezidiv bei Nierenzellkarzinom in der Vena cava inferior
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Rezidiv bei Nierenzellkarzinom in der Vena cava inferior:
Assoziationen und Differentialdiagnosen zu Rezidiv bei Nierenzellkarzinom in der Vena cava inferior:
