cystic lymphangioma of the pancreas
Pancreatic lymphangiomas are benign lesions that are often found incidentally during cross-sectional imaging for another reason.
For a broader discussion, please refer to the parental article on lymphangioma.
Clinical presentation
More common in adults (in contrast to lymphangiomas in the head and neck, which are more common in children). Account for approximately 1% of abdominal lymphangiomas. More common in women
Pathology
Lymphangiomas are thought to arise from a congenital blockage of regional lymphatic ducts. They can be pancreatic or peripancreatic.
They may contain serous, serosanguinous, or chylous fluid. Cyst walls are lined with endothelial cells (immunoreactive with VIII-R AG, CD31, and D2-40; negative for CD34).
Radiographic features
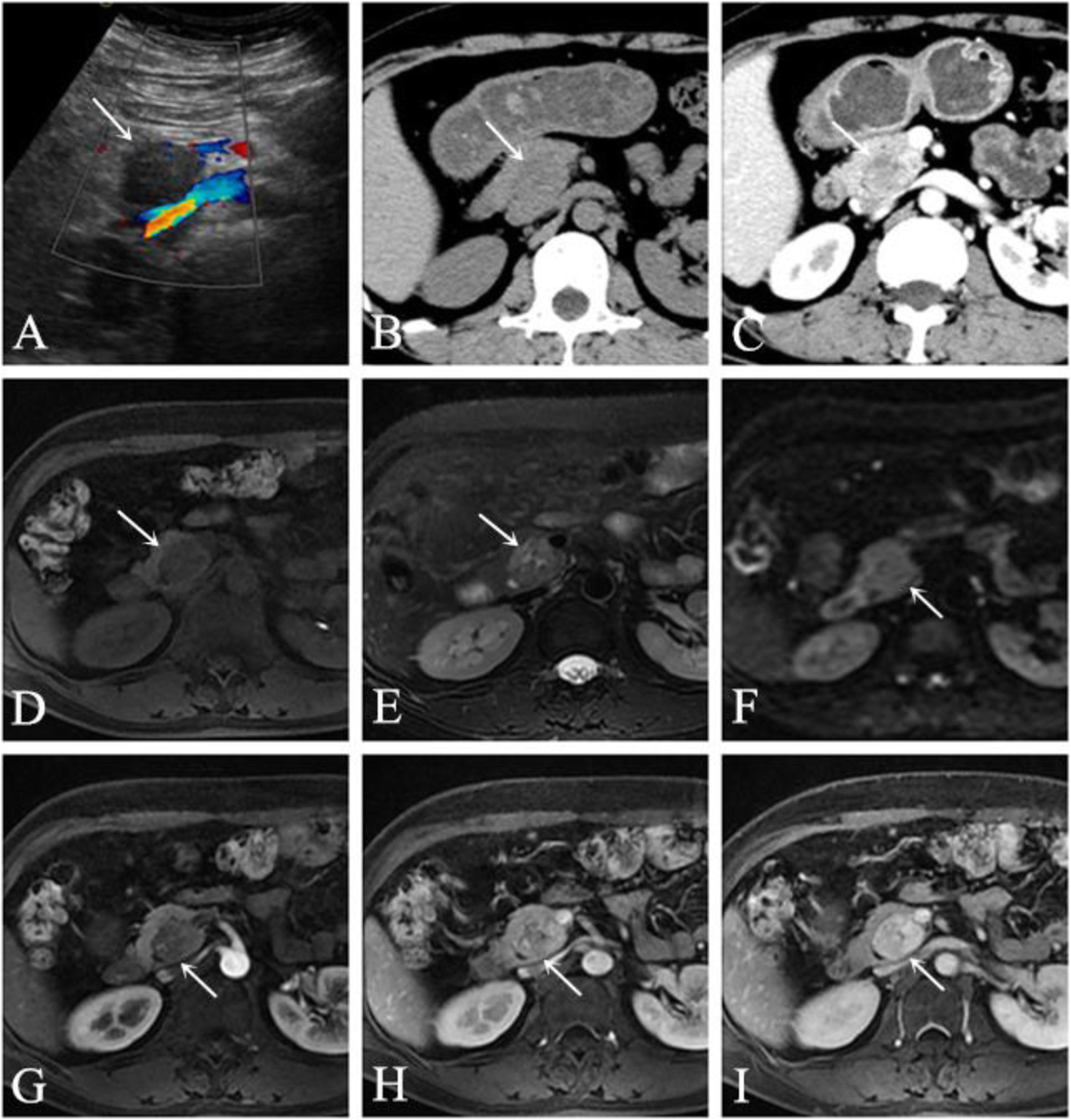
US
- multiple hypoechoic or anechoic cysts
- contents may be echogenic
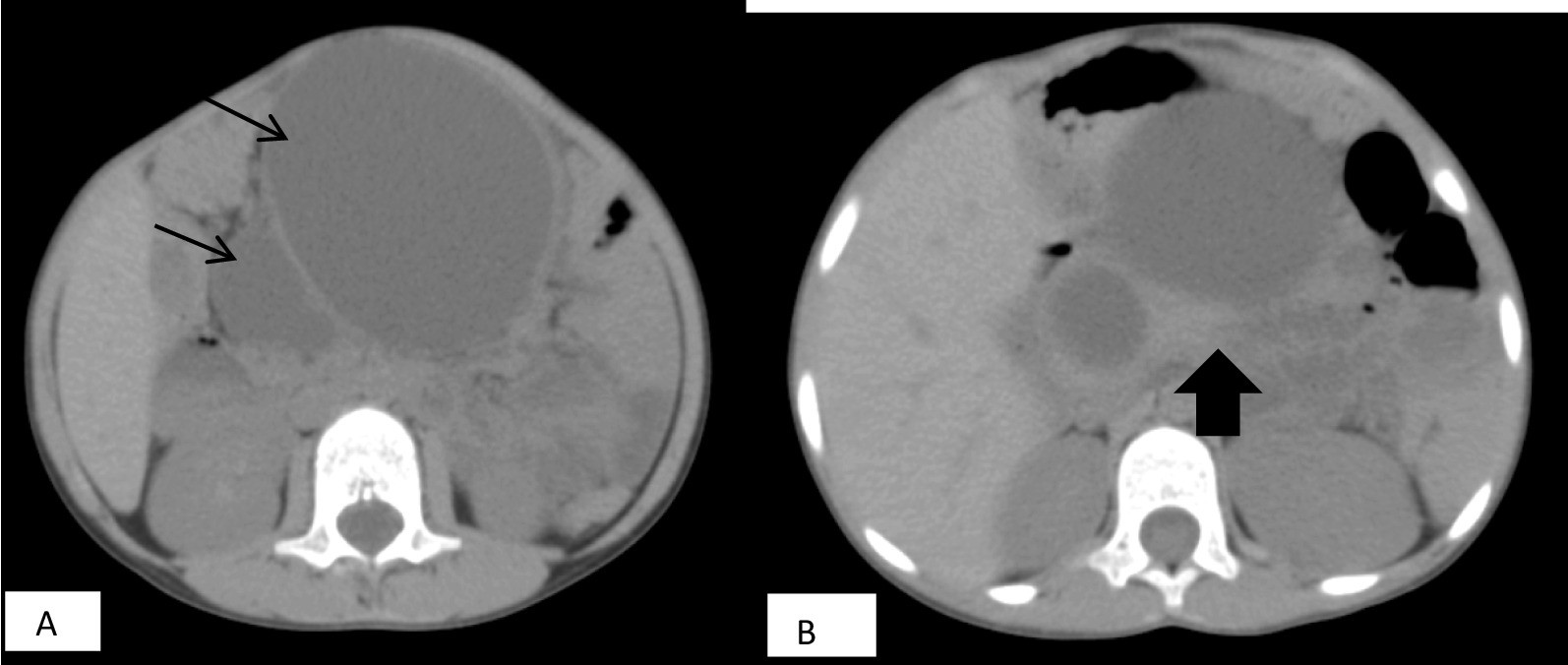
CT
- multilocular and multiseptated (occasionally unilocular)
- homogeneously hypoattenuating, may be fat attenuation
- phleboliths may be present
- they can become quite large
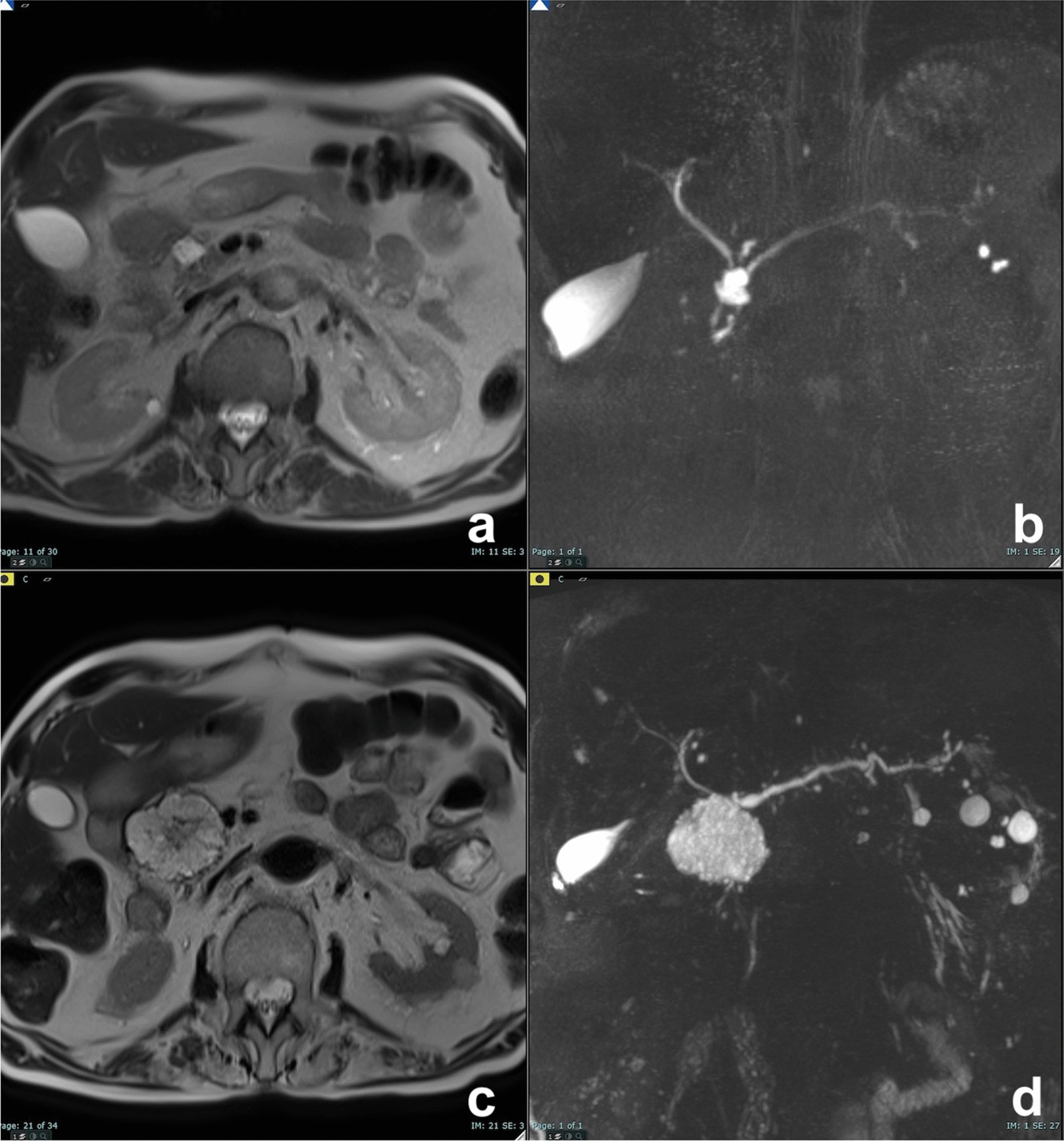
MRI
- T1: hypointense
- T2: hyperintense
- multiseptated, lobulated
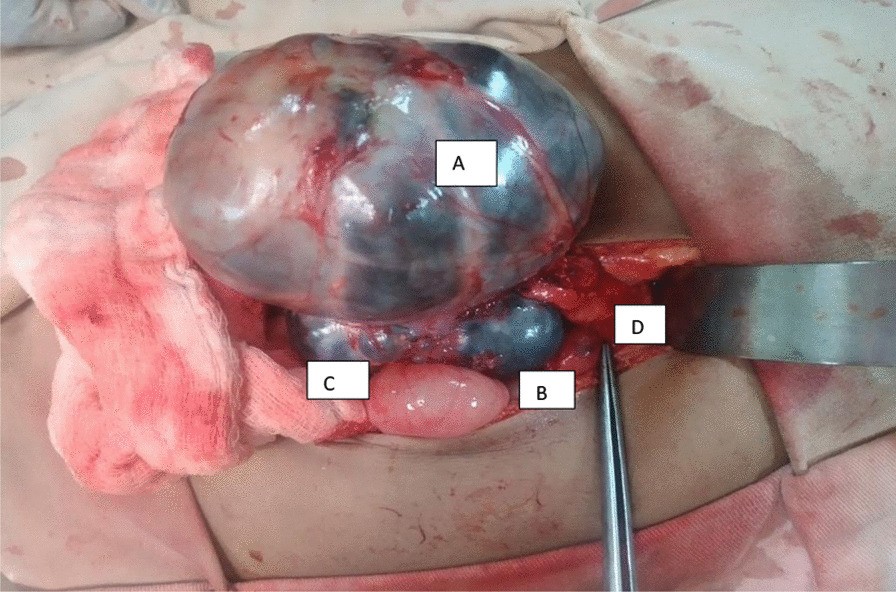
Treatment and prognosis
Endoscopic ultrasound (EUS) with cyst fluid aspiration is probably the best way to confirm a pancreatic lymphangioma (it has an elevated triglyceride level).
Treatment is not usually necessary but may be excised if locally invasive.
Differential diagnosis
- side branch intraductal papillary mucinous neoplasm (IPMN)
- if a connection to the main duct of the pancreas can be found, this entity becomes much more likely
- a mucinous lesion of the pancreas
- oligocystic serous cystadenoma of the pancreas
- acute peripancreatic fluid collection / pseudocyst
- a history of pancreatitis is usually present
- pancreatic neuroendocrine tumor
Practical points
a pancreatic lymphangioma should not have any enhancing component. If an enhancing component is present, it is more prudent to consider one of the neoplastic entities on the differential
finding fat attenuation in the cystic lesion helps to separate pancreatic lymphangioma from other entities on the differential
- if a lymphangioma becomes secondarily infected, it may be difficult to distinguish it from a more aggressive lesion
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Lymphangiom des Pankreas:
Assoziationen und Differentialdiagnosen zu Lymphangiom des Pankreas: