Endgliedfrakturen














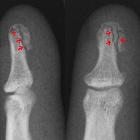
Distal phalanx fractures are among the most common fractures in the hand.
They represent > 50% of all phalangeal fractures and frequently involve the ungual tuft.
They are frequently related to sports, with lesions such as the mallet finger and the Jersey finger. When associated with a crush injury, open fracture is more likely.
Radiographic features
Plain radiographs form the mainstay of imaging distal phalanx fractures. The presence or absence of an intra-articular component, degree of comminution, and fracture displacement should be assessed when formulating a report.
Fracture rotation can be difficult to assess radiologically and is best assessed on clinical examination. Fractures with significant radiological comminution and/or extensive soft tissue injury should be clinically and radiologically reviewed for open fracture.
Treatment and prognosis
The majority of distal phalanx fractures are minimally displaced and may be treated conservatively. Closed fractures are generally stable, especially when they do not involve the articular surface. A mallet splint is often used in these cases.
Fractures at the base of the distal phalanx are often unstable due to the fact these are the insertions sites for both the flexor and extensor tendon, however splinting of these fractures, granted they are closed has favorable outcomes .
As in all cases of trauma, the importance of recognition of open distal phalanx fractures is due to the increased risk of contamination and, hence, infection. Extensive wound irrigation, antibiotic cover, and tetanus booster prophylaxis must be considered to mitigate this risk. Surgery for nailbed repair and/or Kirschner wire fixation will be required in more complex cases.
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Endgliedfrakturen:
Assoziationen und Differentialdiagnosen zu Endgliedfrakturen: 