extrakranielles Aneurysma der Arteria vertebralis
Treatment of
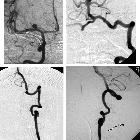
Extracranial Vertebral Aneurysm Associated with Two Intracranial Aneurysms—A Case Report: Figure 1. Preoperative angiograms. Upper-left corner: right carotid angiogram, anteroposterior projection, revealing a round aneurysm located on the proximal segment of the middle cerebral artery. Upper-right corner: left vertebral angiogram, anteroposterior projection, showing an irregular end-basilar aneurysm. Lower-left corner: left vertebral angiogram, left anterior oblique projection, demonstrating an aneurysm on the cervical segment of the artery (V2 segment). Lower-right corner: left vertebral angiogram, lateral projection, showing the vertebral aneurysm and the spinal collateral artery (arrow).
Chronic
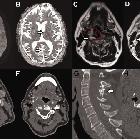
fusiform extracranial vertebral artery aneurysm with recurrent posterior circulation emboli: Case report and review of the literature: A and B: Multiple foci of restricted diffusion (white arrow), with corresponding low ADC value in the posterior circulation involving the right occipital lobe, left thalamus and cerebellum (not shown), in keeping with acute embolic infarction. Older non-restricting foci of embolic infarction were also evident on T2 sequences (not shown). C: T2 weighted sequence of the neck at the C4 vertebral level demonstrating an abnormal right vertebral artery (red broken line) with a central flow void and abnormal circumferential thick mixed T2 signal material (white arrow). Maximal diameter of the fusiform aneurysm was up to 35mm. D: T2 weighted sequence of the neck at the C4 vertebral level five years prior to presentation confirming significant growth (white arrow) of the right vertebral artery (red broken line). E and F: CT angiography demonstrated a grossly abnormal right vertebral artery measuring up to 5cm in diameter. The aneurysm demonstrated thick thrombus lining the lumen (black arrow) with areas of fissuring and crenulation. The contralateral left vertebral artery was of normal calibre and appearances (white arrow). G: Sagittal bone window reconstruction of CT demonstrates abnormal appearance to the spinous processes (white arrow) of C2 to C4 consistent with historic trauma. H: Axial CT at C3 level shows a grossly expanded right foramen transversarium consistent with a chronic process of fusiform aneurysm formation (black arrow).

Chronic
fusiform extracranial vertebral artery aneurysm with recurrent posterior circulation emboli: Case report and review of the literature: A: Digital subtraction angiography (DSA)(anterior-posterior view) confirmed a chronic fusiform aneurysmal right vertebral artery with areas of saccular dilatation (grey arrow). The distal V3 segment of the vertebral artery (white arrow) and intra-cranial basilar artery were normal (black arrow). B: DSA (lateral view) endovascular embolization was performed with distal micro-vascular plug and platinum coils (white arrow). Contrast stagnation can be seen in the areas of saccular dilatation. C: Proximal cervical vertebral artery embolization was performed with a single micro-vascular plug (black arrow). D: Pre-embolization angiogram with injection in the left vertebral artery demonstrates normal appearances with no opacification of the right posterior inferior cerebellar artery territory (PICA). E: Post-embolization retrograde flow of contrast from the left vertebral artery fills the intra-dural right vertebral artery (white arrow) and perfuses the right PICA (black arrow).
extrakranielles Aneurysma der Arteria vertebralis
Siehe auch:


 Assoziationen und Differentialdiagnosen zu extrakranielles Aneurysma der Arteria vertebralis:
Assoziationen und Differentialdiagnosen zu extrakranielles Aneurysma der Arteria vertebralis: