fibrolamelläres HCC


Fibrolamellar hepatocellular carcinoma is a distinct histological variant of hepatocellular carcinoma characterized on microscopy by laminated fibrous layers between the tumor cells. It is important as it has different demographics and risk factors compared to 'standard' hepatocellular carcinomas.
Epidemiology
Typically these tumors occur in young adults (20 to 40 years of age) without gender predilection. Unlike HCCs they do not have an association with cirrhosis, alcoholism, or hepatitis B/C infection .
Clinical presentation
Presentation is non-specific, with constitutional symptoms and occasionally gynecomastia due to elevated estrone levels. Hepatomegaly is usually evident as these masses are typically large.
Pathology
These tumors are well-differentiated and well-circumscribed, with a dense fibrotic background . The tumor cells are arranged in cords that are separated by sheetlike fibrous bands arranged in a parallel or lamellar distribution : hence the name, fibrolamellar.
Fibrolamellar carcinomas often do not produce alpha fetoprotein (AFP).
Radiographic features
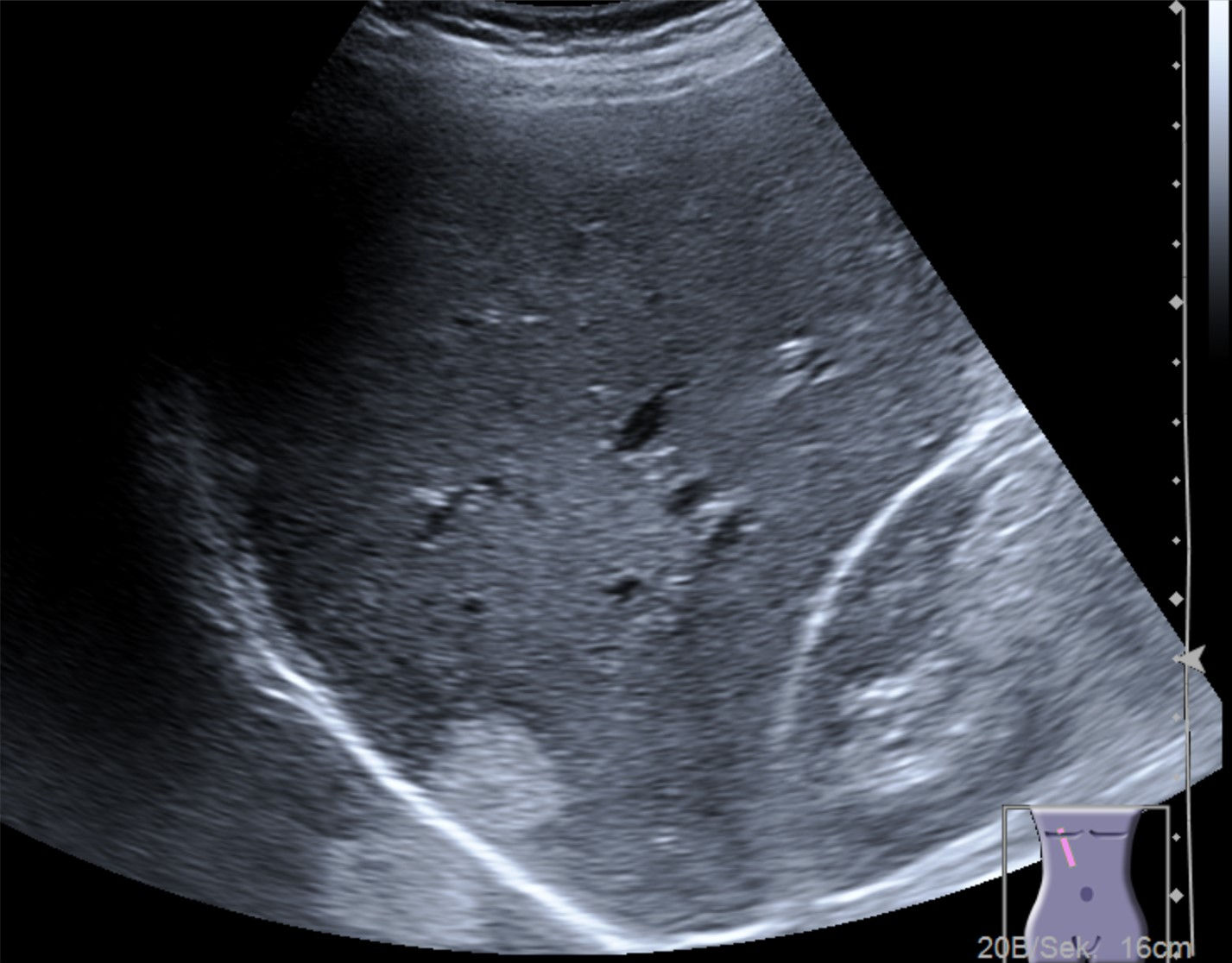
Ultrasound
- variable sonographic appearance
- contrast-enhanced ultrasound
- arterial phase:
- heterogeneous enhancement
- portal venous phase:
- decreased echogenicity relative to background liver ("wash out")
- arterial phase:
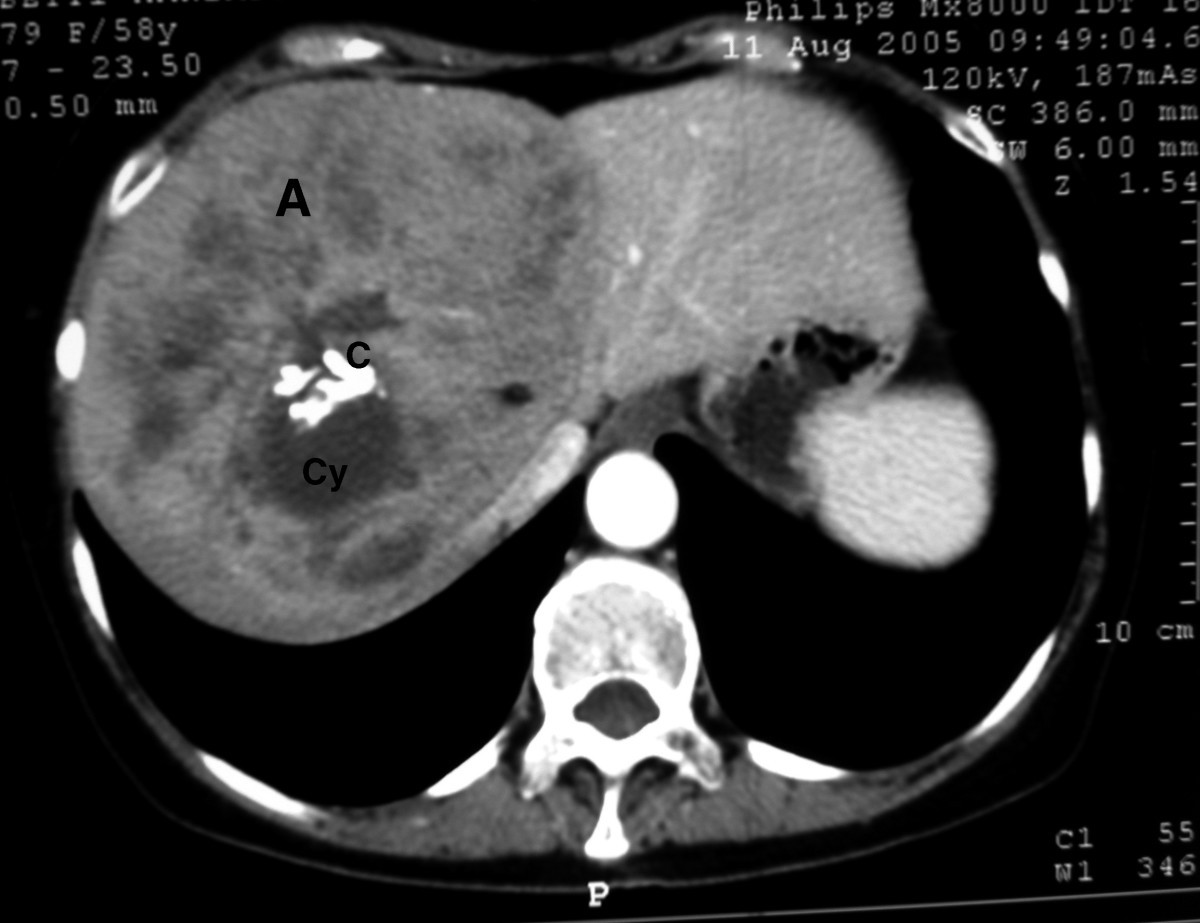
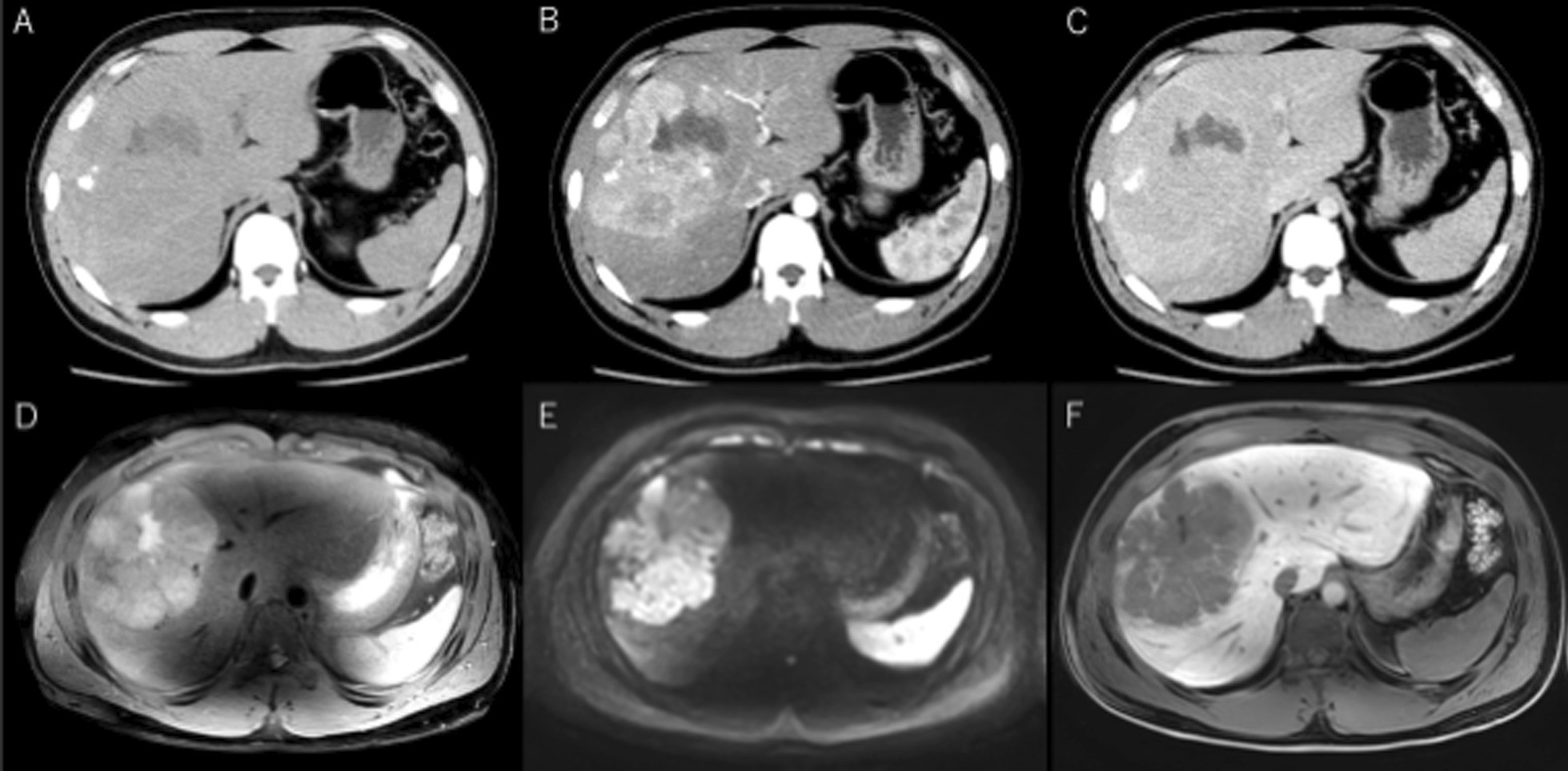
CT
Fibrolamellar HCCs typically are single large tumors with dense fibrotic bands forming a central scar (seen in ~75% of cases), which make it resemble focal nodular hyperplasia (FNH). A few small calcifications are seen in 35-65% of cases. Regional (hepatic hilum) nodal enlargement is seen in ~50% of cases. Enhancement is usually arterial. The central scar typically shows persistent enhancement on delayed contrast enhanced CT.
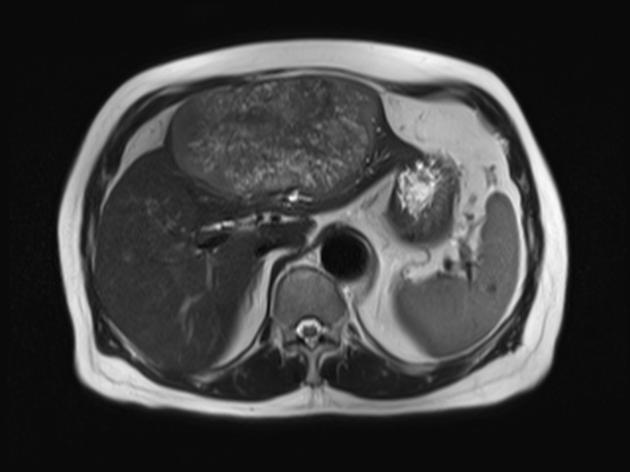
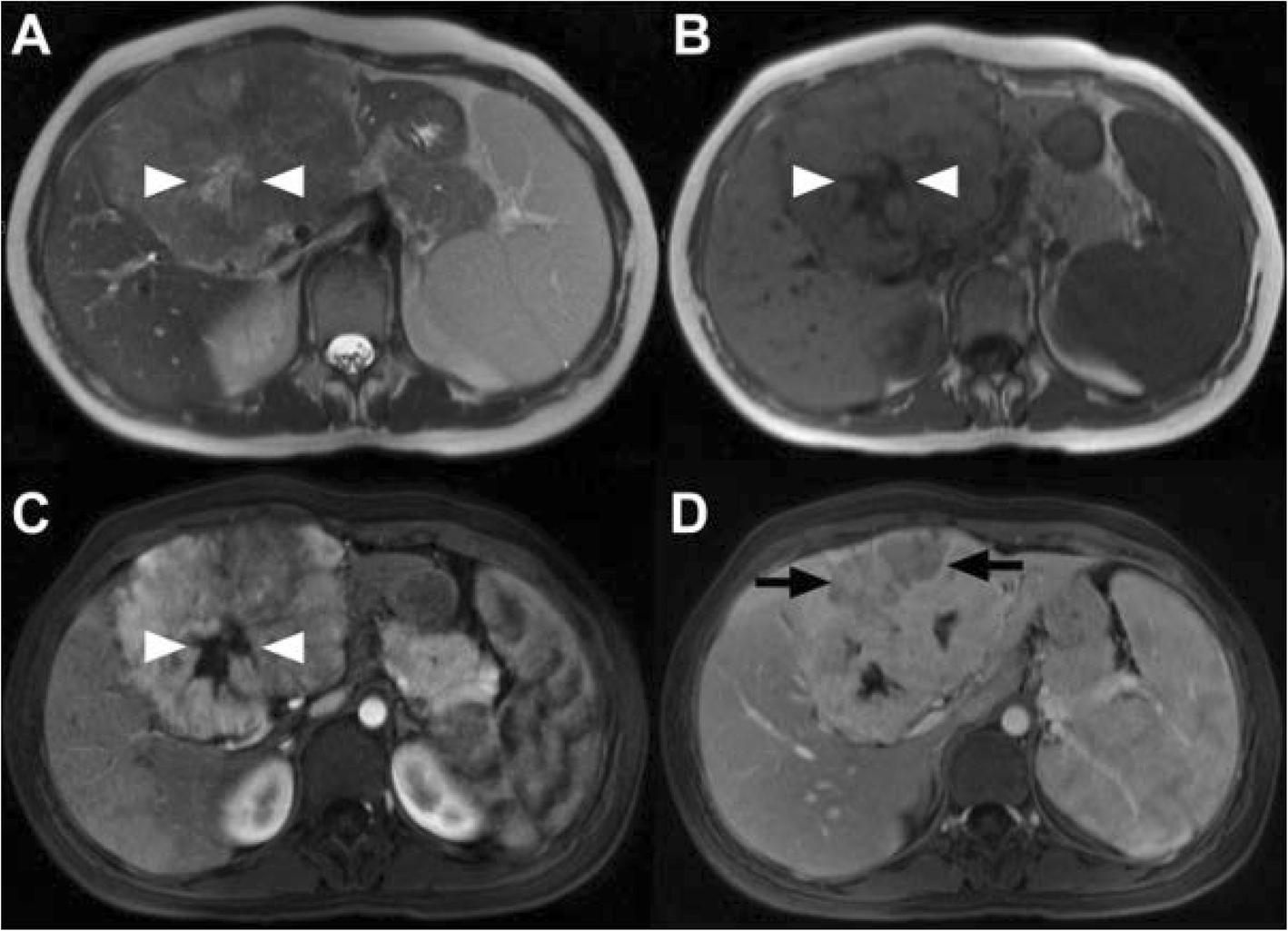
MRI
The central scar, when present, is usually hypointense on all sequences. Occasionally it may be T2 hyperintense mimicking FNH . Fibrolamellar HCCs do not contain fat, and thus do not lose signal on out of phase imaging .
Signal characteristics
- T1: typically iso to hypointense to the liver
- T2: hypo to slightly hyperintense
- T1 C+ (Gd)
- arterial phase: heterogeneous enhancement
- portal venous / delayed phase: iso to hypointense
- T1 C+ (Primovist / Eovist)
- liver-specific contrast agent uptake has not been reported in the hepatobiliary phase
Nuclear medicine
Technetium-99m sulfur colloid scans (taken up by Kupffer cells) are useful as these tumors will not accumulate the agent, whereas focal nodular hyperplasia does.
Treatment and prognosis
Fibrolamellar carcinoma is less aggressive than HCC but usually, due to lack of symptoms until it becomes sizable, and often a lack of secretion of AFP, stage at presentation tends to be advanced.
Resection is the treatment of choice, with a resulting 5-year survival of 76%. This compares favourably to generic HCC which, even when resectable, has a 5-year survival of only 37-56%.
If unresectable, this tumor is universally fatal.
Differential diagnosis
General imaging differential considerations include:
- hepatocellular carcinoma (HCC)
- different demographics: underlying liver disease
- less likely to have calcification or central scar
- elevated AFP
- focal nodular hyperplasia (FNH)
- uptake of Tc-99m sulfur colloid usually present
- scar is often hyperintense on T2
- less heterogeneity and fewer calcifications than fibrolamellar HCC
- will retain liver-specific contrast agent (e.g. Eovist); this has not been reported in HCC
- hepatic adenoma
- uptake of Tc-99m sulfur colloid in up to 25% of cases
- hepatic metastasis
- large liver hemangioma
- peripheral pooling, delayed central filling-in with contrast
- may also have central scar if large
Siehe auch:
- Leberhämangiom
- hepatozelluläres Karzinom
- Lebermetastasen
- Leberadenom
- Fokale noduläre Hyperplasie
- primäre Lebertumoren
- fibrolamelläres Leberkarzinom im Kindesalter
- fibrolamelläres Leberkarzinom mit Verkalkungen
und weiter:


 Assoziationen und Differentialdiagnosen zu fibrolamelläres hepatozelluläres Karzinom:
Assoziationen und Differentialdiagnosen zu fibrolamelläres hepatozelluläres Karzinom: