mechanische kreislaufunterstützende Devices bei akutem Herzversagen

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure.

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. a Illustration demonstrates the position of the intra-aortic balloon pump placed from the femoral artery. b Illustration demonstrates the normal position of the Impella CP LV support system. The device is implanted from the femoral artery. Impella pump can also be implanted through the axillary artery or aorta. c Illustration demonstrates the normal position of the Protek Duo in the main pulmonary artery and the Impella CP LV support system. In this illustration, we see use of two separate devices for biventricular support

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Intra-aortic balloon pump (IABP). Chest AP radiograph (a) demonstrating the upper radiopaque marker (white arrow) projecting over the aortic knob superior to the carina. This is the expected position based on radiography. Abdomen AP radiograph (b) in the same patient demonstrates the IAPB with the inferior radiopaque marker (white arrow) projecting over the L1-L2 Intervertebral space, which is low. Oblique coronal CT (c) demonstrates the IAPB in the descending aorta. The radiopaque marker is visible within the descending aorta about 5 cm from the origin of left subclavian artery. Sagittal CT abdomen image (d) demonstrates the low position of the IABP with its inferior radiopaque marker (black marker) below the level of the diaphragm at the level of the L1–L2 Intervertebral space. This can be seen when there is anatomic-to-balloon length mismatch

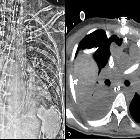
CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Complication from low IABP. AP chest radiograph (a) of a patient with an intra-aortic balloon pump. The upper radiopaque marker is below the carina (white arrow) which suggests a low position. Sagittal image (b) of a contrast enhanced chest and abdomen CT at the level of the celiac trunk and superior mesenteric artery (SMA) origin demonstrates high grade obstruction of the SMA and celiac trunk ostia by the distended IABP. Axial CT image (c) identifies complication from hypoperfusion: pneumatosis and contained perforation of the cecum (white arrow), due to the hypoperfusion from the high grade celiac trunk and SMA ostial occlusion. (IABP—Intra-aortic balloon pump)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Malposition of axillary IABP. AP chest radiograph with contrast limited adaptive histone equalization (CLAHE) filter demonstrating an axillary approach IABP (a, b). The IABP is malpositioned with the upper marker in the brachiocephalic artery (white arrow on image a). The black arrow indicates the location of the sheath. The inflated balloon is seen in the aortic arch and upper descending aorta. The inferior marker is within the descending aorta (dashed arrow). b AP chest radiograph after attempted advancement of the IABP, the superior marker is malpositioned and is now in the ascending aorta (white arrow). The inferior marker is in the descending aorta (dashed arrow). (IABP = Intra-aortic balloon pump, CLAHE = Contrast limited adaptive histone equalization)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. AP chest radiograph (a) and coronal CT (b) demonstrating a correctly positioned transaxillary Impella device. The outlet port is within the ascending aorta (white arrow) and the inlet port is projecting over the left ventricle (dashed arrow). The inlet of Impella CP should be 3.5 cm below the aortic annulus. The outlet should be in the ascending aorta. The pigtail portion is angled toward the LV apex away from the ventricle wall without mitral obstruction. (LV—left ventricle)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Malposition of Impella pump. AP Chest radiograph with CLAHE filter (a) with an Impella CP device with the outlet port in the aortic arch (white arrow) and the inlet port at the level of the aortic valve (dashed arrow). Contrast enhanced CT coronal image (b) at the level of the LVOT demonstrates high/proximal placement of Impella device with the blood inlet port at the level of the aortic valve. Contrast is seen only in the aorta but not in the left ventricle. This is due to backfilling from the VA ECMO cannula in the femoral artery. (CLAHE—contrast limited adaptive histogram equalization, LVOT—left ventricle outflow tract, VA ECMO—veno-arterial extracorporeal membrane oxygenation)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Malposition of Impella device. AP Chest radiograph with CLAHE filter (a) demonstrates a left ventricle Impella device with its tip projecting over the left ventricle (black arrow). Axial contrast enhanced CT (b) demonstrating the pigtail portion of the Impella device is entangled within the papillary muscle apparatus (black arrow). This finding is not detected on radiograph but can be identified on a CT. (CLAHE—contrast limited adaptive histogram equalization)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Complication of Impella device. Axial non-contrast CT in a patient on transfemoral Impella device demonstrates medial displacement of the intimal calcification. This is consistent with an acute aortic dissection

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Complication from Impella. AP Chest radiograph with a left ventricle Impella device (a). The inlet port of the Impella is not in expected location on this radiograph, outlet port is much below the carina (white arrow) and the pigtail portion is coiled in the left ventricle cavity (white dashed arrow). The pigtail portioned is coiled, this is a sign of malposition. This can indicate entrapment within the papillary muscle apparatus. Non-contrast coronal CT at the level of the LVOT (b) confirms low positioned of the Impella device. The tip of the device has perforated the left ventricular wall (white arrow) and high density fluid can be seen in the pericardium, compatible with hemopericardium. (LVOT—Left ventricle outflow tract)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Chest radiograph with CLAHE filter in a patient with an Impella RP for right ventricle support. The pigtail portion in the outflow is in the main pulmonary artery. The inlet is in the IVC (white arrow). (CLAHE—contrast limited adaptive histogram equalization, IVC–inferior vena cava)

CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Chest radiograph demonstrating a right-sided placement of a LV Impella 5.5. This device was placed intraoperatively through a pulmonary artery graft. The inflow is located in the right ventricle and the outflow is located in the main pulmonary artery (white arrow) through the graft. The inlet and outlet directions can be changed depending on need to optimize flow. Note. There is no pigtail portion in the Impella 5.5 which helps differentiate this device. (LV—Left ventricle)
CT and chest
radiography in evaluation of mechanical circulatory support devices for acute heart failure. Protek Duo for right ventricle support. AP Chest radiograph with CLAHE filter after Protek Duo placement (a) demonstrating right basilar and mid-lung opacities. The outlet cannula portion should be in right ventricle and the inner portion within the pulmonary artery. In this case, the outlet cannula tip is within the right pulmonary artery. This can cause asymmetric perfusion and edema. Axial CT (b) in mediastinal window demonstrates asymmetric pulmonary opacities, right pleural effusion and a hemothorax (white arrow). (CLAHE—contrast limited adaptive histogram equalization)
mechanische kreislaufunterstützende Devices bei akutem Herzversagen
Siehe auch:


 Assoziationen und Differentialdiagnosen zu mechanische kreislaufunterstützende Devices bei akutem Herzversagen:
Assoziationen und Differentialdiagnosen zu mechanische kreislaufunterstützende Devices bei akutem Herzversagen:
