mucinous breast carcinoma





Mucinous carcinoma of the breast, also known as colloid breast carcinoma, is a subtype of invasive ductal carcinoma (IDC). They account for about ~ 2% (range 1-7% ) of breast cancers.
Epidemiology
It tends to occur in older women where a prevalence of as much as 7% is found among women 75 years or older, whereas the prevalence is only 1% in women younger than 35 years .
Clinical presentation
If palpable, they tend to manifest as soft masses.
Pathology
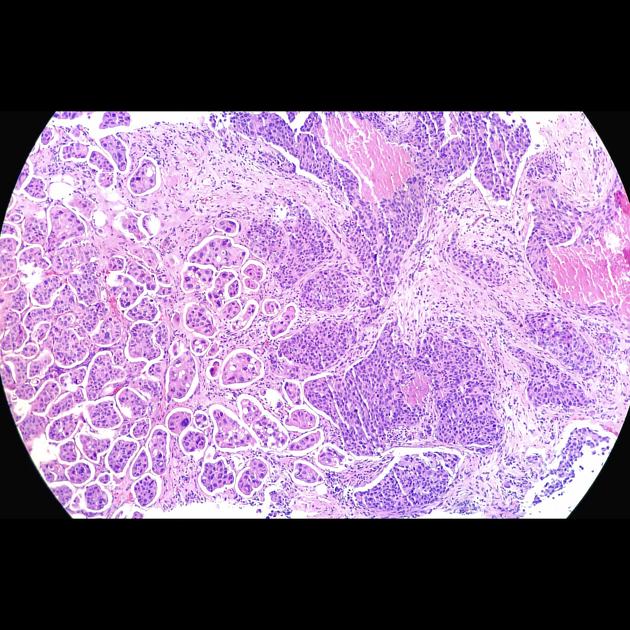
At pathological examination, the dominant feature is the presence of mucin within and surrounding cancer cells. The mucin to cell ratio can vary from lesion to lesion. A core biopsy specimen usually gives a gelatinous appearance. Microscopically, it is formed by large mucin lakes surrounded by mucus-producing cancer cells.
Histologically it is divided into two broad types:
- hypocellular type A or pure mucinous breast cancer: entire tumor consists of well-differentiated carcinoma cells with excessive extracellular mucin surrounding them. The growth pattern is often expanding, cellularity and mitotic activity are low, and cell atypia is not very prominent. The margin of the tumor is usually well demarcated
- hypercellular type B or mixed mucinous breast cancer: tumor also contains variable areas of DIC-NOS component. They are devoid of extracellular mucin. This type is more likely to be infiltrative and carries much worse prognosis
Radiographic features
Majority of well-marginated breast masses are benign but approximately 10–20% of breast malignancies also could be well-circumscribed such as mucinous tumors; others include papillary, medullary, and metaplastic carcinomas as well as malignant phyllodes tumors. Because of different patterns of mammogram and ultrasound, both should be performed in all cases of MCB and in some equivocal cases breast MRI is of great value.
Mammography
The presence of mucin results in a low-density and relatively well-defined lobular mass. Sometimes they may have partly faded or obscure margins. Up to 20% of lesions can be occult on mammography . Calcification can be rare in pure mucinous types.
Ultrasound
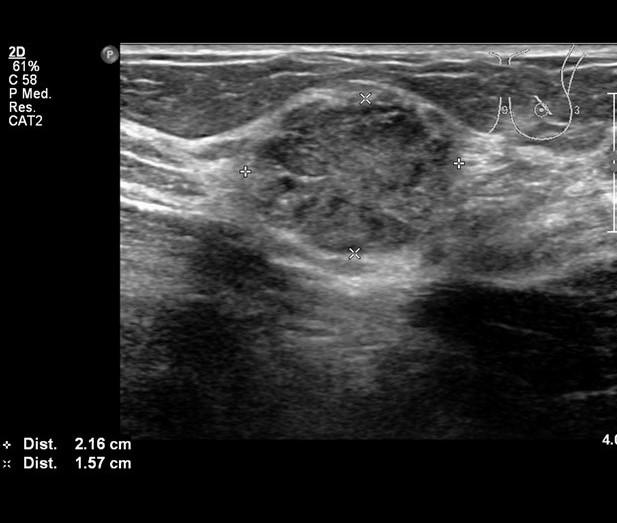
At ultrasound, mucinous carcinomas often display mixed echogenicity with mixed solid and cystic components. Posterior acoustic enhancement is common. As times the lesion can be isoechoic to breast tissue on ultrasound which can make diagnosis difficult .
Sonographically, mixed cystic and solid components, distal enhancement, and microlobulated margins are commonly found in mucinous carcinomas. Homogeneity on sonography is associated with the pure type of MCB, in which margins are usually well defined, and the tumor is iso-echogenic relative to the fat surrounding the breast tissue on ultrasound. A mixed MCB tends to be more hypoechoic.
Breast MRI
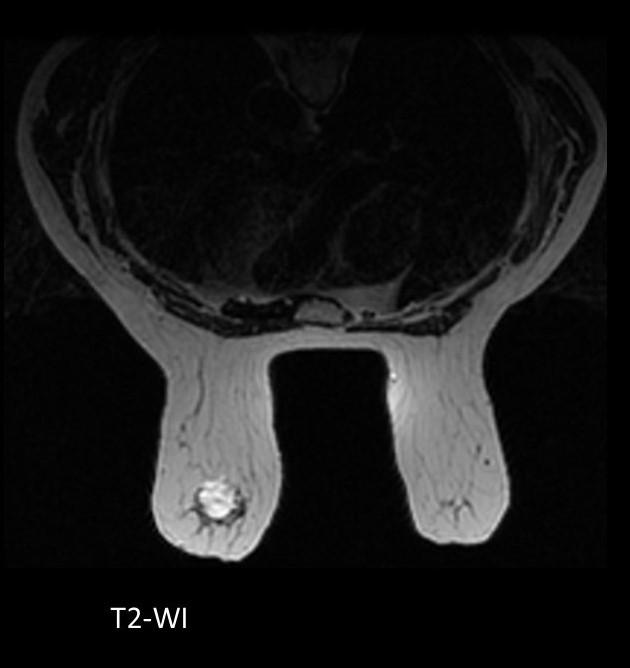
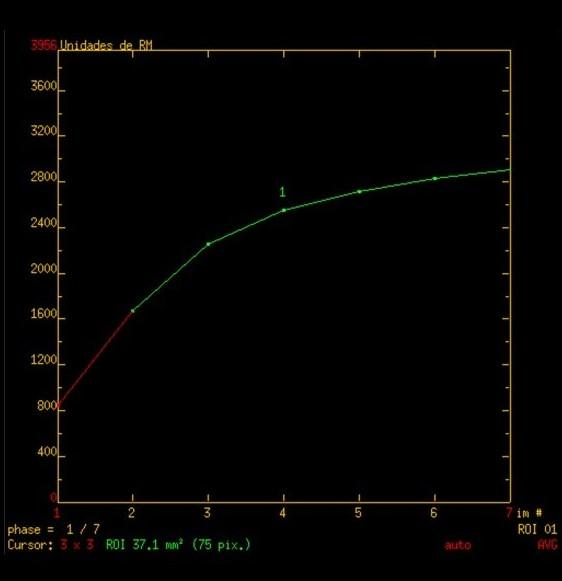
On MRI, they are one of the few cancers that have very high signal intensity on T2-weighted images which relates to the water component in mucin. When compared with other malignant breast tumors, they show lower signal intensity on DWI and increased ADC values. On postcontrast images, benign-appearing kinetics with gradual and persistent enhancement is typical and so they can be easily mistaken for a benign lesion.
PET/CT
PET/CT may help to differentiate pure from mixed mucinous carcinoma and to evaluate the aggressiveness of the tumor.
Treatment and prognosis
A pure mucinous subtype carries a relatively good prognosis compared to other adenocarcinomas: 5-year survival 95% (stage 2), 75% (stage 3), 35% (stage 4). Overall the tendency to metastasize is less than for other types of cancer (e.g. invasive ductal carcinoma not otherwise specified). Mixed MCB has more aggressive behavior.
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu invasives muzinöses Mammakarzinom:
Assoziationen und Differentialdiagnosen zu invasives muzinöses Mammakarzinom: