retropharyngealer Abszess


















Retropharyngeal abscess is a potentially life-threatening infection involving the retropharyngeal space which requires prompt diagnosis and aggressive therapy.
Epidemiology
Retropharyngeal abscesses are most frequently encountered in children, with 75% of cases occurring before the age of 5 years, and often in the first year of life . This is likely due to the combination of prominent retropharyngeal nodal tissue and frequency of middle ear and nasopharyngeal infections. There may be a slight male predilection .
Occasionally retropharyngeal infections can result from a variety of other miscellaneous causes, including trauma/foreign body injection . Immunocompromised patients are also at increased risk of developing a retropharyngeal abscess.
Clinical presentation
Presentation is variable. In some instances, children present with non-specific symptoms including generalised irritability, fever and reticence to eat. In other cases, features are more pronounced, including drooling, fever, neck swelling, limited range of motion and stridor, and clinically the presentation may be reminiscent of epiglottitis . This is particularly the case in infants . Palpable cervical lymph nodes may also be present .
Alternatively, and uncommonly in developed countries, patients may present with complications resulting from the extension of the infection to adjacent spaces (see below).
Pathology
Retropharyngeal abscesses are thought to result as a complication of a primary infection elsewhere in the head and neck including the nasopharynx, paranasal sinuses, or middle ear (e.g. otitis), which in turn drain lymph to (among others) the retropharyngeal lymph nodes. Other potential sources include oral cavity and oropharyngeal infections (tonsillitis, pharyngitis), discitis/osteomyelitis, and penetrating trauma .
Suppuration of these nodes then leads to an extension of the infection to the surrounding tissues which are bounded by facial planes resulting in an unimpeded potential craniocaudal spread from the base of skull to the mediastinum.
Aetiology
Causative agents are variable, and include :
- group A Streptococcus
- S. aureus
- H. influenzae
- anaerobic organisms, e.g. Bacteroides, Peptostreptococcus, and Fusobacterium
- M. tuberculosis: in endemic areas or in the immunocompromised
Radiographic features
Plain radiograph
Radiographs, which have the advantage of being able to be obtained with the patient sitting, demonstrate soft tissue swelling posterior to the pharynx, with a widening of the prevertebral soft tissue. This appearance cannot be distinguished from a prevertebral abscess, and careful evaluation of the vertebral bodies and disc spaces is important.
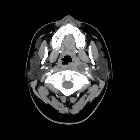
CT
CT is excellent at evaluating the neck and is able to do so in a short time (much faster than an MRI) which is an important factor when imaging patients with potential narrowing of the airway. Scans should be obtained with contrast to allow differentiation of fluid collections from phlegmonous thickening (retropharyngeal cellulitis).
It is important to note however that CT has a not insignificant rate of both false positive (10%) and false negative (13%) rate with respect to detecting pus, and as such surgical exploration may need to be carried out on the basis of clinical presentation .
It is important to differentiate retropharyngeal abscess from retropharyngeal oedema. True abscess will usually have a peripherally enhancing rim with a centrally hypodense collection, expansion of the retropharyngeal space, and may contain locules of gas .
MRI
MRI has superior contrast resolution than CT and is able to interrogate the retropharyngeal space with a number of imaging sequences including diffusion.
- T1: central low to intermediate signal
- T2: central high signal
- T1 C+ (Gd): peripheral enhancement
- DWI: increased values, indicative of restricted diffusion
Careful assessment of the relationship of the collection with the carotid sheath and evaluation for potential vascular complications (thrombosis, pseudoaneurysm formation) is essential .
Treatment and prognosis
Treatment is similar in principle to that of other infected collections usually requiring both surgical drainage (usually performed via a transoral route) and intravenous antibiotics. In some instances, antibiotics alone may suffice when collections are small .
With a prompt diagnosis, appropriate antibiotics and drainage when necessary, almost all patients recover uneventfully.
Complications
Serious complications in developed nations with prompt access to imaging and antibiotic are uncommon, however, complacency needs to be avoided as retropharyngeal can lead to potentially life-threatening complications including :
- posterior extension to pre-vertebral space, discitis osteomyelitis, epidural abscess
- lateral extension involving carotid artery (haemorrhage, pseudoaneurysm, thrombosis, stenosis) and jugular vein (thrombosis)
- anterior compression and compromise of the airway
- inferior extension into the mediastinum resulting in mediastinitis (e.g. via involvement of the danger space, carotid sheath or visceral space)
- systemic dissemination and development of sepsis
- Grisel syndrome
- Lemierre syndrome
Differential diagnosis
- retropharyngeal cellulitis: i.e. same pathology but no abscess formation
- retropharyngeal oedema: hypoattenuation without a well defined or enhancing rim
- prevertebral abscess: usually secondary to discitis osteomyelitis
- retropharyngeal haematoma
- blood density/intensity on CT/MRI
- Capps triad
- usually in adults
- retropharyngeal effusion secondary to acute calcific prevertebral tendinitis
- no marginal enhancement
- calcification may be seen in the longus capitits and longus colli muscles
- mass involving retropharyngeal space: e.g. haemangioma, tumour
- retropharyngeal pseudothickening (especially in young children i.e. short neck)
- excessive neck flexion
- swallowing
- expiration
Siehe auch:
- verbreiterter prävertebraler Weichteilschatten
- kalzifizierende Tendinitis des Musculus longus colli
- Retropharyngealraum
- retropharyngeale Raumforderung
- retropharyngeales Hämatom
- Grisel-Syndrom
- parapharyngealer Abszess
- retropharyngeales zystisches Hygrom
- Osteomyelitis im Clivus
- retropharyngeal effusion
- spontanes retropharyngeales Hämatom
und weiter:


 Assoziationen und Differentialdiagnosen zu retropharyngealer Abszess:
Assoziationen und Differentialdiagnosen zu retropharyngealer Abszess: