Colonic pseudo-obstruction








Colonic pseudo-obstruction (also known as Ogilvie syndrome) is a potentially fatal condition leading to an acute colonic distention without an underlying mechanical obstruction. It is defined as an acute pseudo-obstruction and dilatation of the colon in the absence of any mechanical obstruction.
Epidemiology
Numerous causes have been identified, and the demographics of affected patients generally reflect these, with elderly unwell patients being most frequently affected . Usually seen in people over 60 years of age and there is male predilection .
Clinical presentation
Patients usually present with constipation, nausea, vomiting and abdominal distension. Pseudo-obstruction can present with a sudden painless enlargement of the proximal colon accompanied by distension. Bowel sounds are normal or high-pitched, but should not be absent.
Despite the absence of mechanical obstruction, patients can nonetheless go on to bowel necrosis and perforation (especially if dilatation is severe) which in turn can go on to become generalized peritonitis .
Pathology
Pseudo-obstruction is related to decreased parasympathetic activity.
Risk factors include:
- trauma
- burns
- recent surgery
- medications
- opioids
- phenothiazines
- clozapine
- respiratory failure
- electrolyte disturbances
- diabetes mellitus
- uremia
Radiographic features
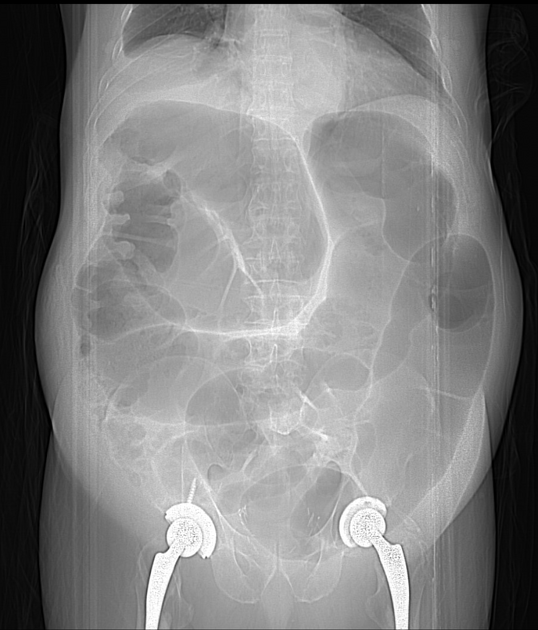
Plain radiograph
Findings can be identical to a mechanical large bowel obstruction .
Fluoroscopy
A single contrast/water-soluble enema demonstrates the absence of any mechanical obstruction.
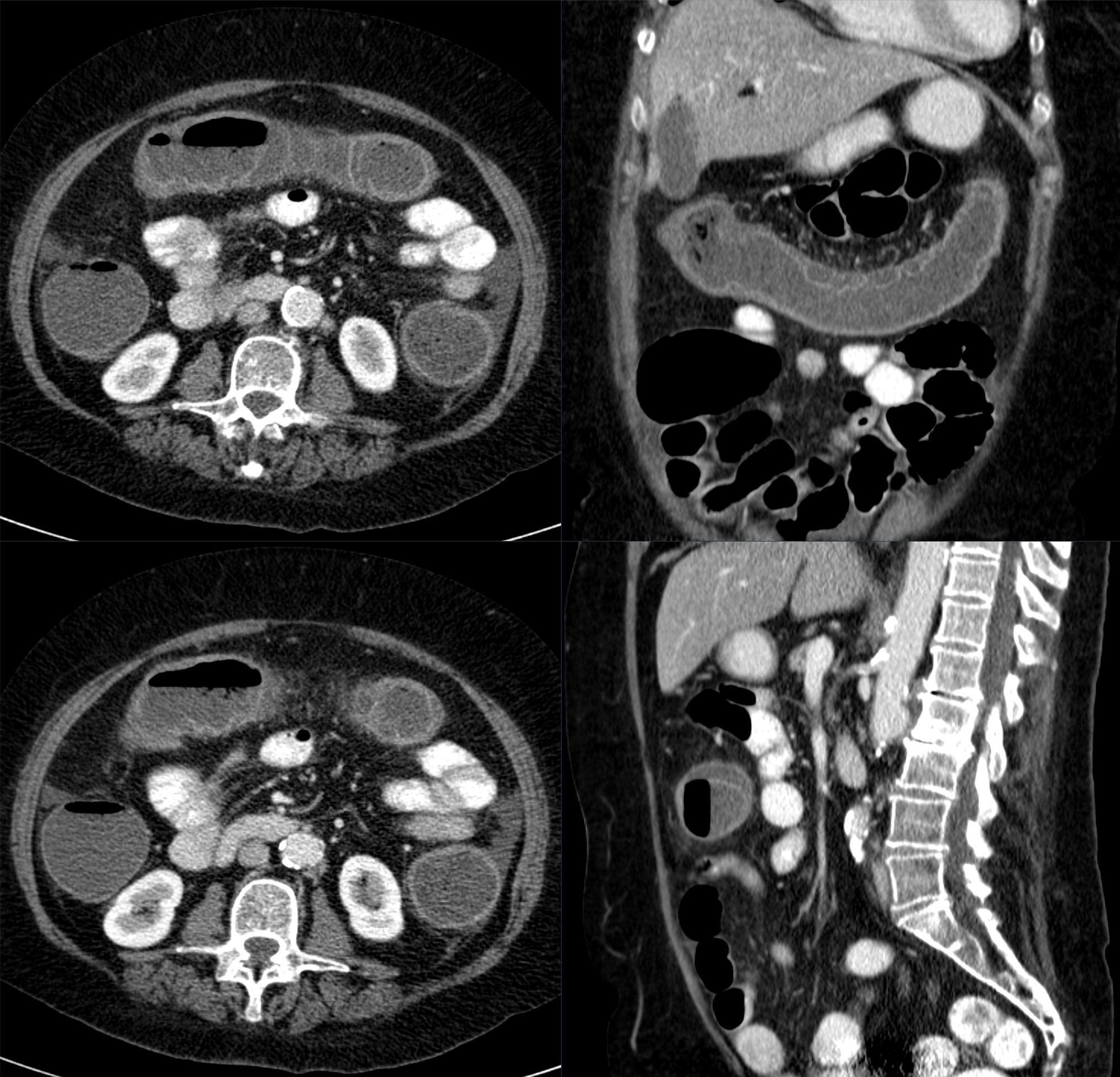
CT
The hallmark of colonic pseudo-obstruction is the presence of dilatation of the large bowel (often marked) without evidence of an abrupt transition point or mechanically obstructing lesion.
It is important to note, however, that a gradual transition point is frequently present, usually at or near the splenic flexure .
Treatment and prognosis
Treatment involves correction of the underlying disorder and correction of any biochemical abnormalities. Medical treatment options include anticholinesterases like neostigmine and antibiotics like erythromycin.
Decompression with a rectal tube (endoscopic decompression) or careful colonoscopy may be effective . In severe cases, surgical or fluoroscopy-assisted cecostomy is necessary, or even occasionally a percutaneous endoscopic colostomy (PEC).
Complications
- cecal perforation: decompression is usually undertaken if the caliber is more than 9-12 cm
History and etymology
It was initially described by the British general surgeon Sir W (William) Heneage Ogilvie (1887-1971) in 1948 .
Differential diagnosis
General imaging differential considerations include:
- adynamic ileus
- no transition point
- often history has a cause for the ileus, e.g. surgery
- small bowel is also often dilated
- mechanical large bowel obstruction
- abrupt transition point often with an identifiable obstructing lesion
- toxic megacolon secondary to Clostridioides difficile colitis
- C. difficile infection is usually preceded by antibiotic use or chemotherapy and is therefore usually encountered in unwell, hospitalized patients with significant co-morbidity
- bowel wall thickening usually a prominent feature
- ischemic colitis
- usually bowel wall is thickened, but can be thinned and dilated
- absent/poor wall enhancement
- usually involves vascular territories
- sigmoid volvulus and cecal volvulus
- transition point evident
- whirlpool sign of the twisted mesentery
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Ogilvie-Syndrom:
Assoziationen und Differentialdiagnosen zu Ogilvie-Syndrom: