Adenoidal hypertrophy (children)

















Adenoidal hypertrophy or enlargement in children is common and due to an increase in the size of the adenoids. For adenoidal enlargement in adults, which is much rarer and usually pathological, please see the separate article, adenoidal hypertrophy (adults).
Clinical presentation
- nasal congestion: adenoid facies
- chronic or recurrent otitis media due to their proximity to the Eustachian tubes
- swallowing difficulties
- speech anomalies (hyponasal speech)
- rhinorrhea
- sleep-disordered breathing
Pathology
Although present at birth, they are usually invisible until age 3 to 6 months. They can grow until about age 6, then involute through adulthood. Enlargement is pathological when they encroach on the nasopharyngeal airway, and this usually does not occur until age 1 to 2 years.
Etiology
Both inflammatory and infectious causes should be considered. Common infectious causes include:
- Haemophilus influenzae
- group A beta-hemolytic Streptococcus
- Staphylococcus aureus
- Moraxella catarrhalis
- Streptococcus pneumoniae
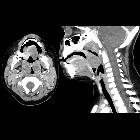
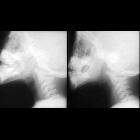
Radiographic features
Plain radiograph
The lateral neck x-ray is the main imaging study. The size of the adenoids is less of a consideration than the degree to which they encroach on the nasopharyngeal airway:
- if no adenoidal tissue after age 6 months, suspect an immune deficiency
- if enlarged adenoids persist well after childhood, suspect lymphatic malignancy
Treatment and prognosis
Management options include:
- waiting until they spontaneously involute
- surgical removal
Indications for an adenoidectomy include:
- enlargement causing nasal airway obstruction
- recurrent or persistent otitis media in children aged 3 to 4 or older; it should be taken into account that treating otitis media resolves the resultant hearing impairment as well
- recurrent or chronic sinusitis
Siehe auch:


 Assoziationen und Differentialdiagnosen zu hypertrophe Tonsillen des Pharynx:
Assoziationen und Differentialdiagnosen zu hypertrophe Tonsillen des Pharynx:

