Developmental Venous Anomaly


































Developmental venous anomaly (DVA), also known as cerebral venous angioma, is a congenital malformation of veins which drain normal brain. They were thought to be rare before cross-sectional imaging but are now recognized as being the most common cerebral vascular malformation, accounting for ~55% of all such lesions.
A DVA is characterized by the caput medusae sign of veins draining into a single larger collecting vein, which in turn drains into either a dural sinus or into a deep ependymal vein. The appearance has also been likened to a palm tree.
Epidemiology
DVAs are very common as incidental finding, with an estimated prevalence of 2.5-9% on contrast-enhanced MRI scans .
Clinical presentation
Developmental venous anomalies are usually incidental findings. However, patients can present with intracranial hemorrhage (1-5%). An association has also been described with ischemic stroke and epilepsy .
Pathology
The etiology of developmental venous anomalies remains uncertain but may relate to arrested development of venous structures . Histologically they consist of a number of abnormally thickened veins with normal feeding arteries and capillaries.
Location and classification
The most common locations are:
- frontoparietal region (36-64%) , usually draining towards the frontal horn of the lateral ventricle
- cerebellar hemisphere (14-27%) draining towards the fourth ventricle
However, DVAs can be seen anywhere, draining either superficially or deep.
Associations
- lesions are usually solitary (75%) , except in blue rubber bleb nevus syndrome
- ~20% (range 8-33%) of cases are associated with cavernous malformations and are referred to as mixed vascular malformations (MVM)
- venous malformations of the head and neck
- cortical dysplasia (uncommon)
Radiographic features
Developmental venous anomalies are seen on both CT and MRI as a leash of vessels draining towards a central vein.
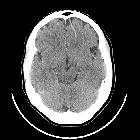
CT
If large, the draining vein may be seen on non-contrast CT and is confirmed with contrast administration as a linear or curvilinear enhancing structure.
Dystrophic calcifications may be seen associated in up to 9.6% of the cases . This can be particularly prominent in the basal ganglia and thalami resulting in unilateral calcification.
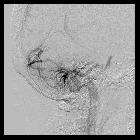
Angiography (DSA)
Angiographically the caput medusae appearance (collection of dilated medullary veins converge in an enlarged transcortical or subependymal collector vein) is pathognomonic and seen only in the venous phase. Arterial phase appears normal although late capillary blush may be present. No shunting is present.
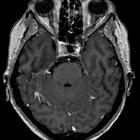
MRI
Developmental venous anomalies are often visible on most sequences but can be subtle and are most easily seen on postcontrast T1 sequences and susceptibility weighted imaging (SWI). If there is an associated cavernous hemangioma, then susceptibility weighted sequences will be most sensitive to this component.
Additionally, in ~10% of cases, high T2 signal will be seen in the surrounding white matter; this may be due to gliosis, edema or leukoaraiosis .
SWI is the preferred sequence in venous anomalies and proved to have better detectability of venous structures than conventional T2*-weighted imaging. Signals on SWI are not compromised by low-velocity venous flow. Therefore, SWI has successfully demonstrated low-flow vascular formations such as DVA. The signal intensity of veins will be low on SWI images but will vary on phase imaging depending on the vendor. It will, however, be the same as other veins and the opposite of calcification.
Treatment and prognosis
If isolated developmental venous anomalies require no treatment. If part of a mixed vascular malformation then treatment will be predicated on the other component. Informing the surgeon of the presence of a DVA is, however, essential as cautery of the collecting vein can lead to venous infarction of the brain parenchyma it drains.
When isolated, developmental venous anomalies have a very low complication rate (0.15% per annum) mainly from spontaneous thrombosis of the collecting vein leading to venous infarction and hemorrhage.
A more recent study has demonstrated that in exceedingly rare cases, the DVA can become symptomatic by various vascular complications. The authors suggested identification of the underlying pathomechanism by MR and DSA for proper management. The importance of the preserved integrity of the DVA itself still holds true .
Differential diagnosis
Generally, the appearances will be typical and no differential should be offered. In some instances, imaging appearances may be atypical or be confounded by concurrent pathology (e.g. hemorrhage). In such cases it is worth considering:
- arteriovenous malformation
- dural sinus thrombosis or dural arteriovenous fistula with collateral transparenchymal drainage
- Sturge-Weber syndrome with leptomeningeal angiomatosis
- demyelination may also have enlarged medullary veins
Practical points
- think of an associated cavernoma when a developmental venous anomaly is found in the context of an intraparenchymal hemorrhage investigation, as isolated DVAs rarely bleed
- developmental venous anomalies can be subtle on many MRI sequences; T1 C+ and SWI are most sensitive
Siehe auch:
- Sinus durae matris
- Sinusthrombose
- Arteriovenöse Malformation
- Sturge-Weber-Krabbe-Syndrom
- Kavernom
- zerebrale Kavernome
- kapilläre Teleangiektasien des ZNS
- Caput medusae Zeichen bei DVA (developmental venous anomaly)
- vierter Ventrikel
- Demyelinisierende Erkrankung
- intrakranielle vaskuläre Malformationen
- mixed vascular malformation
- palm tree sign
- Developmental Venous Anomaly eingeblutet
- MVM
und weiter:
- zerebrale arteriovenöse Malformation
- animal and animal produce inspired signs
- Ponsblutung
- neuroradiologisches Curriculum
- Caput medusae
- cerebral malformation
- vaskuläre Anomalien im Pons
- Klassifikation zerebraler vaskulärer Malformationen
- zerebrale venöse Malformationen
- venöses Angiom Kleinhirn
- Developmental Venous Anomaly im Pons
- Anomalien der craniellen venöse Drainage
- Developmental Venous Anomaly mit Verkalkungen
- DVA Gehirn
- hemorrhagic developmental venous anomaly
- intracranial haemorrhage from developmental venous anomaly
- angiogram of DVA
- cerebellar developmental venous anomaly


 Assoziationen und Differentialdiagnosen zu Developmental Venous Anomaly:
Assoziationen und Differentialdiagnosen zu Developmental Venous Anomaly: