double aortic arch



















Double aortic arches are the most common symptomatic type of the aortic arch variant. It may account for up to 50-60% of vascular rings.
Clinical presentation
Double aortic arch is mostly diagnosed in childhood due to symptoms related to esophageal and/or tracheal obstruction. Respiratory symptoms can be more common in infancy or early childhood while adult patients complain of difficulties in swallowing rather than respiratory difficulties due to tracheal development.
Pathology
This anomaly is caused by persistence of the right and left embryonic fourth aortic arches, which results in formation of a vascular ring from the splitting of the ascending aorta into two limbs that pass to either side of the trachea and esophagus (both of which get encircled), which then join as a single descending aorta.
When the minor arch is markedly hypoplastic or atretic (incomplete double aortic arch), the affected segment tends to be almost always distal to the left subclavian artery .
Subtypes
- right dominant arch: ~75-80%
- codominant arch: ~5%
- left dominant arch: ~25%
Associations
It is rarely associated with congenital heart disease .
Radiographic features
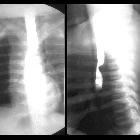
Plain radiograph
Right-sided aortic arch indenting the trachea and increase right paratracheal soft tissue thickness. Lack of air column in the thoracic portion of the trachea is sometimes seen.
Fluoroscopy: barium swallow
Contrast swallow studies are more helpful and demonstrate:
- classic "reverse S" indentation of the contrast column on frontal view produced by an upper indentation of the right-sided aortic arch and the lower indentation is by the left-sided aortic arch
- posterior indentation on lateral view produced by the encircling posterior arch (mostly right-sided aortic arch component)
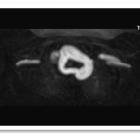
CT and MRI
Contrast-enhanced cross-sectional imaging is required to confirm the diagnosis and also to delineate details of anatomy in particular right or left arch dominance for surgical planning.
Treatment and prognosis
Surgical intervention with tracheostomy from the side of descending aorta and division of the minor (smaller) arch and ligamentum arteriosum is indicated for symptomatic patients. In appropriate cases, surgical planning is directed toward transection of either the smallest arch (if both arches are patent) or an atretic arch segment.
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu doppelter Aortenbogen:
Assoziationen und Differentialdiagnosen zu doppelter Aortenbogen:
