enostosis












Enostoses, also known as bone islands, are common benign sclerotic bone lesion which usually represent incidental findings. They constitute a small focus of compact bone within cancellous bone. Enostoses can be seen on radiographs, CT, and MRI, and are considered one of the skeletal “don’t touch” lesions.
Pathology
The etiology of enostoses is not definitively known. They are most likely congenital or developmental in nature and are thought to represent either hamartomatous lesions or failure of osteoclastic activity during bone remodeling .
Although they have at times previously been referred to as benign bone tumors (in part due to occasional increased activity on bone scintigraphy), enostoses have been removed from the WHO classification of bone tumors .
Location
Bone islands may occur anywhere in the skeleton, although there is some predilection for pelvis, long bones, spine and ribs.
Associations
- osteopoikilosis: multiple bone islands
Radiology
Plain radiograph / CT
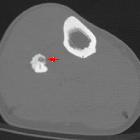
Enostoses are commonly seen as small round or oval foci of dense bone within the medullary space. The appearance of radiating spicules - "thorny radiation" or "fingers" - at the margins that blend with the surrounding trabeculae is classic.
In diaphyseal bone, the long axis of a bone island typically parallels the long axis of the involved bone. In the metaphysis, and other regions where trabeculation is not as linearly organized, the bone islands are typically more spherical.
The size of a bone island is typically <1 cm, although large bone islands may occur, particularly in the pelvis, and when greater than 2 cm in maximal dimension are called giant bone islands . Sometimes a slow increase in size is seen in bone islands over time.
A sclerotic bone lesion can be diagnosed as a bone metastasis versus bone island if its mean attenuation is < 885 HU and maximum attenuation is < 1060 HU with a 95% sensitivity and a 96% specificity for both values .
MRI
Low signal intensity on all sequences (compatible with compact bone).
Nuclear medicine
There is usually no technetium-99m MDP uptake, and a normal bone scan can exclude an osteoblastic metastasis or osteosarcoma. However, low-grade scintigraphic activity has sometimes been reported in histologically proven enostoses .
Treatment and prognosis
Consider biopsy if the lesion grows 50% in one year or 25% in six months .
Differential diagnosis
In the vast majority of cases, bone islands have a pathognomonic appearance. Larger lesions may sometimes pose a diagnostic dilemma, particularly in the setting of known malignancy.
Imaging differential considerations include:
- osteoblastic metastasis
- osteoma
- osteoid osteoma
- low-grade osteosarcoma
- benign osteoblastoma
See also
Siehe auch:
- osteoblastische Knochenmetastasen
- Osteom
- Osteoid-Osteom
- Osteosarkom
- Kompaktainsel Becken
- Osteopoikilose
- solitary sclerotic bone lesion
- Kompaktainsel der Skapula
und weiter:
- vertebrale Metastasen
- radiologisches muskuloskelettales Curriculum
- Knochentumoren
- spinale Metastasen
- bones
- verkalktes Enchondrom
- primary tumours of the spine
- Sklerosierung der Klavikula
- bone-forming tumours
- osteoid lesions
- Osteoidosteom der Wirbelsäule
- Knocheninsel
- bone island in vertebral body
- knochenbildende Tumoren


 Assoziationen und Differentialdiagnosen zu Kompaktainsel:
Assoziationen und Differentialdiagnosen zu Kompaktainsel: