hypothenar hammer syndrome

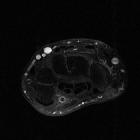



Hypothenar hammer syndrome occurs from trauma to the distal ulnar artery or proximal portion of superficial palmar arch as a result of repetitive trauma to the hypothenar eminence. Originally described in patients using hammers and screwdrivers, it is also seen in various athletes such as basketball, handball, tennis and golf players.
Clinical presentation
- cold senstation and pain in the palm
- Raynaud syndrome
- tender hypothenar eminence
- ischemia of (usually) fourth and fifth fingers
- positive Tinel sign (due to ulnar nerve compression)
- positive Allen test
Pathology
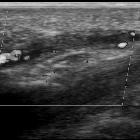
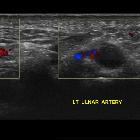
It may be caused by any repetitive compression or blunt trauma to this region. The ulnar artery is particularly vulnerable as it passes over the hook of hamate. Trauma to the artery may result in dissection, stenosis, occlusion or false aneurysm formation. This may be complicated by distal thromboembolism.
Radiographic features
Angiography
- “corkscrew” or beaded irregular appearance distal ulnar artery
- aneurysm formation
- occlusion of the ulnar artery segment overlying the hook of the hamate
- occluded or under-filled distal digital arteries in an ulnar artery distribution
Treatment and prognosis
Overall management strategy is controversial. Non-surgical treatment is considered sufficient, particularly in the setting of vasospasm with adequate collateral circulation.
Conservative options include;
- smoking cessation
- avoidance of further trauma
- padded protective gloves
- cold avoidance
- calcium channel blockers (e.g. nifedipine, diltiazem)
- antiplatelet agents or anticoagulation
- local care of fingers with necrosis
- pentoxifylline: for viscosity reduction
See also
Siehe auch:
- Arcus palmaris superficialis
- Raynaud-Syndrom
- Thenar-Hammer-Syndrom
- pseudotumoröse Weichteilläsionen von Hand und Handgelenk
- arterielle Durchblutungsstörungen der Hand
- Hoffmann-Tinel-Zeichen
- thrombosis of the ulnar artery
und weiter:


 Assoziationen und Differentialdiagnosen zu Hypothenar-Hammer-Syndrom:
Assoziationen und Differentialdiagnosen zu Hypothenar-Hammer-Syndrom:
