Listerien-Rhombenzephalitis








Listeria rhombencephalitis is a particular form of listerial encephalitis that affects primarily the hindbrain (brainstem and cerebellum). Listeria monocytogenes, an anaerobic bacterium, is cited as the most common etiology for rhombencephalitis, typically seen in the elderly, and resulting in significant morbidity and mortality.
Please refer to the article on rhombencephalitis for a general discussion of that entity.
Epidemiology
The majority of listerial rhombencephalitis reported cases occurred in previously healthy adults . In contrast listerial cerebritis is rare and encountered mostly in the setting of profound immune compromise .
Clinical presentation
Encephalitis caused by Listeria are often misdiagnosed initially due to a nonspecific prodrome (fever, headache, nausea and vomiting) and unusual meningeal signs .
Patients with rhombencephalitis later develop a spectrum of symptoms due to brainstem involvement, such as multiple cranial nerve palsies (occur in ~75% of all cases) or cerebellar deficits, long-tract motor and/or sensory deficits, ataxia, nystagmus, vertigo, facial numbness, dysphagia, persistent hiccuping, and respiratory failure (~41%) .
CSF
- increased leukocyte count (usually due polymorphonuclear cells)
- increased protein
- normal glucose levels
It is difficult to isolate the agent: the bacillus can be cultured from blood in 61% and from CSF in 41% .
Pathology
Etiology
Listeria monocytogenes is an anaerobic and gram-positive bacillus.
Radiographic features
Beam-hardening artifacts limit the visualization of the brainstem on CT images (initial CT of the brain often gives normal results) and MRI is the imaging modality of choice for the assessment of patients with suspected pathology in that anatomic location. The protocol should include contrast.
Subcortical abscesses in the thalamus, pons and medulla are common in rhombencephalitis caused by this bacteria .
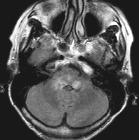
MRI
- T1: hypo- to isointense lesion
- T2/FLAIR: hyperintense
- DWI: hyperintense/hypointense on ADC map
- T1 C+:
- linear cranial nerve enhancement
- ring enhancement (abscess)
- heterogeneous if extensive inflammation
Treatment and prognosis
It is reported to have a high mortality (~50%) and frequent serious sequelae for survivors (~60%) .
Survival is strongly related to the timely use of appropriate antibiotics: usually ampicillin or penicillin combined with gentamicin for a period of at least six weeks .
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Listerien-Rhombenzephalitis:
Assoziationen und Differentialdiagnosen zu Listerien-Rhombenzephalitis: 