Non-seminomatous germ cell tumors











Non-seminomatous germ cell tumors (NSGCTs) are one of the main groups of germ cell tumors (the other being seminoma). Although they are made up of distinct histological entities, in general, they have similar radiographic appearances. They can, however, be found widely in the body, with variable imaging features, pathology, treatment and prognosis. As such they are discussed separately.
This article focuses on a general discussion of non-seminomatous germ cell tumors, as well as providing a structure to individual articles.
Epidemiology
They occur in younger patients than seminoma, with a peak incidence in late teens to twenties. They are the most common primary testicular malignancy, accounting for ~60% of cases.
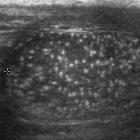
Some consider testicular microlithiasis to be a risk factor for germ-cell tumors, although this is controversial.
Clinical presentation
They tend to be more aggressive than seminomas, and frequently metastasize.
Serological markers
Approximately 70% of non-seminomatous germ cell tumors produce hormonal markers (tumor markers):
- alpha-fetoprotein (AFP): typically elevated in yolk sac tumor
- beta-human chorionic gonadotropin (B-hCG): typically elevated in choriocarcinoma
- lactate dehydrogenase (LDH)
Pathology
Non-seminomatous germ cell tumors can be divided histologically into:
- embryonal cell carcinoma: rare
- choriocarcinoma: rare (carries worst prognosis)
- yolk sac tumor
- teratoma: accounts for 5-10% of germ cell tumors
- mature
- immature
- teratoma with malignant transformation
- mixed germ cell tumor
- is the most common type of NSGCT
- accounts for 40% of all germ cell tumors
- the most common combination is teratoma and embryonal cell carcinoma
See: classification of germ cell tumors.
Radiographic features
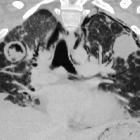
In contrast to seminomas, non-seminomatous germ cell tumors tend to be more heterogeneous on ultrasound and on T2-weighted MR images with frequent cystic areas or calcification. They tend to be more aggressive than seminomas and tunica invasion is common. The appearance of an individual tumor will, of course, vary depending on the location. Please refer to the parent article germ cell tumors for links to specific locations.
Imaging is also essential for the staging of non-seminomatous germ cell tumors which is location dependent. See testicular cancer staging.
Treatment and prognosis
The prognosis of non-seminomatous germ cell tumors is variable and depends on the biological behavior of individual tumors. Prognosis can be inferred from tumor markers, the location of the primary tumor and the presence of metastases .
- good prognosis (all of the following must be true)
- tumor markers
- alpha-fetoprotein <1000 ng/mL
- beta HCG <5000 IU/L
- LDH <1.5x upper limit of normal
- non-mediastinal location of the primary tumor
- no nonpulmonary metastases
These patients are usually treated with orchiectomy followed by chemotherapy (bleomycin, etoposide and cisplatin - BEP regimen).
- tumor markers
- intermediate prognosis (all of the following must be true)
- tumor markers
- alpha-fetoprotein: 1000-10,000 ng/mL
- beta-hCG: 5000-50,000 IU/L
- LDH: 1.5-10x upper limit of normal
- non-mediastinal location of the primary tumor
- no nonpulmonary metastases
These patients are started with chemotherapy cycles and sometimes followed by adjuvant surgery.
- tumor markers
- poor prognosis (any of the following):
- tumor markers
- alpha-fetoprotein: >10,000 ng/mL
- beta-hCG: >50,000 IU/L
- LDH: >10x upper limit of normal
- mediastinal primary tumor
- nonpulmonary metastases present
- tumor markers
Considering a poor prognosis, surgery is usually precluded, and patients are followed with aggressive chemotherapy.
Siehe auch:
- Teratom
- Mikrolithiasis testis
- Chorionkarzinom
- Seminom
- Keimzelltumor
- classification of germ cell tumours
- testicular cancer staging
und weiter:
- mediastinales Teratom
- Hodentumoren
- Seminom des Hodens
- unilateral testicular lesions
- maligne Neoplasien des Hodens
- germ cell tumour classification
- risk factors for testicular germ cell tumour
- Dottersacktumor
- testicular mixed germ cell tumours
- growing teratoma syndrome
- germ cell tumours of the testes
- testicular yolk sac tumour
- testicular germ cell tumours
- Dottersacktumor des Hodens
- Merkspruch Keimzelltumoren


 Assoziationen und Differentialdiagnosen zu nichtseminomatöser Keimzelltumor:
Assoziationen und Differentialdiagnosen zu nichtseminomatöser Keimzelltumor: