osteochondroma


































Osteochondromas are a relatively common imaging finding, accounting for 10-15% of all bone tumors and approximately 35% of all benign bone tumors. Although usually thought of as a benign bone tumor, they may be thought of as a developmental anomaly. They are frequently asymptomatic and have very low malignant potential if sporadic and solitary.
Epidemiology
Osteochondromas develop during childhood (period of most rapid skeletal growth), but once formed remain for the rest of the individual's life. They can present at any age and are most frequently found incidentally.
They are usually sporadic, but can be part of:
- hereditary multiple exostoses (HME): also known as diaphyseal aclasis
- Trevor disease: also known as dysplasia epiphysealis hemimelica
Malignant transformation occurs in the cartilage cap, and is uncommon in sporadic solitary osteochondromas (~1%), whereas in the setting of hereditary multiple exostoses the rate is much higher (5-25%) .
Clinical presentation
Symptomatic presentation is either due to mechanical effects of the lesion, fracture, or malignant transformation.
Mechanical symptoms include:
- impingement upon nearby structures:
- nerve compression
- vascular compression
- reactive myositis
- palpable lump
- bursal formation and bursitis
Fractures occur typically through the neck of pedunculated lesions.
Ongoing growth and or pain after skeletal maturity has been reached is suspicious for malignant degeneration.
Pathology
Osteochondromas are considered a chondroid neoplasm and are primarily a part of the growth plate which separates and continues growing independently, without an associated epiphysis, usually away from the nearby joint. The medullary cavity is continuous with the parent bone, and hyaline cartilage caps them. Osteochondromas can be congenital or occur as a result of previous trauma to the growth plate, including previous irradiation .
Location
They most commonly arise from the appendicular skeleton, especially around the knee :
- lower limb: 50% of all cases
- femur (especially distal): most common: 30%
- tibia (especially proximal): 15-20%
- less common locations: feet, pelvis
- upper limb
- humerus: 10-20%
- less common locations: hands, scapula
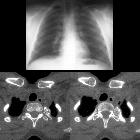
- spine: the posterior elements of the spine are an uncommon but not rare site for these tumors
Radiographic features
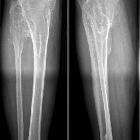
Plain radiograph
An osteochondroma can be either sessile or pedunculated and is seen in the metaphyseal region typically projecting away from the epiphysis. There is often associated broadening of the metaphysis from which it arises. The cartilage cap is variable in appearance. It may be thin and difficult to identify, or thick with rings and arcs calcification and irregular subchondral bone.
New cortical irregularity or continued growth after skeletal maturity has been reached, as well as frankly aggressive features (e.g. bony destruction, large soft tissue component, metastases) are all worrying for malignant transformation.
CT
CT demonstrates the same findings as on radiograph but is better able to demonstrate medullary continuity and the cartilage cap.
Ultrasound
Ultrasound is able to demonstrate the cartilage cap very accurately as a hypoechoic region bounded by bone on its deep surface and muscle/fat superficially.
MRI
MRI is the best imaging modality to assess cartilage thickness (and thus assessing for malignant transformation), the presence of edema in bone or adjacent soft tissues, and visualizing neurovascular structures in the vicinity.
The cartilage cap of osteochondromas appears the same as cartilage elsewhere, with intermediate to low signal on T1 and high signal on T2 weighted images.
A cartilage cap of over 1.5 cm in thickness is suspicious for malignant degeneration .
With intravenous gadolinium administration, enhancement of benign lesions is normally seen in the tissue that covers the cartilaginous cap which is fibrovascular in nature, however, the cartilaginous cap itself should not enhance.
Nuclear medicine
During growth, osteochondromas demonstrate increased uptake on bone scans, but with time they become no more active than normal bone. Presence of increased activity in adulthood should raise the possibility of a complication (e.g. fracture, malignancy).
Treatment and prognosis
As they represent normal growth of a growth plate in an abnormal direction, they often stop growing with the rest of the skeleton .
In most instances, no treatment is required. The osteochondroma can be locally resected for cosmetic or mechanical reasons.
If malignant transformation occurs (~1% in solitary osteochondromas and ~5-25% with hereditary multiple exostoses) then the resultant chondrosarcoma is usually of low grade (67-85% of cases), and surgery is usually curative (70-90%) . Limb-sparing wide local excision usually suffices. The features associated with sarcomatous transformation can be remembered by the mnemonic GLAD PAST :
- growth after skeletal maturity
- lucency (new)
- additional scintigraphic activity
- destruction (cortical)
- pain after puberty
- and
- soft tissue mass
- thickened cartilage cap greater than 1.5cm
Local recurrence is seen in both benign and malignant lesions, due to spillage of cartilage cells into the resection bed. Rates are estimated at 2% and up to 15% respectively .
Differential diagnosis
Imaging differential considerations include:
- hands: bizarre parosteal osteochondromatous proliferation (BPOP): arises from the bone cortex and lacks medullary continuity
- humerus: supracondylar spur: projects towards the elbow joint
- malunited fracture
Siehe auch:
- Multiple kartilaginäre Exostosen
- kartilaginäre Exostose Femur
- Processus supracondylaris
- bizarre parosteale osteochondromatöse Proliferation
- Exostosen des Humerus
- kartilaginäre Exostose Humerus
- Kartilaginäre Exostosen bei Kindern
- sarkomatöse Entartung kartilaginäre Exostose
und weiter:
- Osteoid-Osteom
- Enchondrom
- Chondrosarkom
- Exostose
- Ollier-Syndrom
- WHO-Klassifikation der Tumoren des zentralen Nervensystems
- Chondrom
- Dysplasia epiphysealis hemimelica
- clavicle abnormalities (paediatric)
- radiologisches muskuloskelettales Curriculum
- Exostosen Tibiaschaft
- Tumoren der Thoraxwand
- Knochentumoren
- Turret Exostose
- subunguale Exostosen
- parossales Osteosarkom
- differential diagnosis for metatarsal region pain
- Metachondromatose
- tibial osteochondroma
- cementifying fibroma
- primary tumours of the spine
- paediatric clavicle abnormalities
- chondroide Tumoren
- Tumoren der Wirbelsäule
- madelung deformity associations (mnemonic)
- Osteoidosteom der Wirbelsäule
- kartilaginäre Exostosen Becken
- Exostosen Kniegelenk
- intraspinales Osteochondrom
- kartilaginäre Exostose der Ulna
- sarcomatous degeneration bone exostosis
- osteochondroma metatarsal
- kartilaginäre Exostose des Kalkaneus
- osteochondroma of the thoracic spine: an atypical location
- kartilaginäre Exostose Knorpelkappe
- osteochondroma of the atlas
- distribution of osteochondroma
- solitary osteochondroma of the fibula
- osteochondroma - fractured
- osteochondroma of the rib


 Assoziationen und Differentialdiagnosen zu kartilaginäre Exostose:
Assoziationen und Differentialdiagnosen zu kartilaginäre Exostose: