Pectus excavatum































Pectus excavatum, also known as funnel chest or trichterbrust , is a congenital chest wall deformity characterized by concave depression of the sternum, resulting in cosmetic and radiographic alterations.
Epidemiology
It is the most common chest wall deformity, accounting for approximately 90% of cases, occurs in up to 1 in 300-1000 births and is more frequently seen in males (M:F = 3:1) . The opposite deformity is known as pectus carinatum (pigeon chest).
Clinical presentation
Although usually objectively asymptomatic, many patients report perceived inability to sustain physical activity. This is often associated with significant body-image issues which can have serious implications for affected children . Other than the obvious cosmetic and psychological issues, pectus excavatum is also occasionally associated with:
- mitral valve prolapse
- restrictive pulmonary function test abnormalities
- cardiac functional abnormalities
Pathology
Associations
Although most are sporadic it can be seen in association with:
- Marfan syndrome
- Noonan syndrome
- Ehlers-Danlos syndrome
- neurofibromatosis type I
- myotonic dystrophy
- fetal alcohol syndrome
- homocystinuria
- osteogenesis imperfecta
- congenital scoliosis
- Poland syndrome
Radiographic features
Plain radiograph
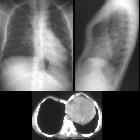
Characteristically demonstrates:
- blurring of right heart border (PA/AP film)
- increased density of the inferomedial lung zone
- horizontal posterior ribs
- vertical anterior ribs (heart-shaped)
- displacement of heart towards the left
- obliteration of the descending aortic interface
- widening of the cardiac silhouette due to compression of heart (PA/AP film)
- sharply defined and more vertically oriented medial breast borders in women, the medial breast margin sign
CT
The diagnosis is obvious on CT with the degree of deformity and mediastinal shift often dramatic.
The Haller index (HI) (maximal transverse diameter/narrowest AP length of chest) is used to assess the severity of incursion of the sternum into the mediastinum. Normal Haller index is 2.5. Significant pectus excavatum has an index greater than 3.25, representing the standard for determining candidacy for repair.
The depression index is computed by identifying the point of maximal depression of the sternum on the CT scan and then drawing a line across the most anterior ribs. This index uses the vertebral body diameter as a correlate to an individual’s size to help normalize for body size and the variable of the thickness of the soft tissue. A measurement is then taken from the mid-sternum perpendicular to this line. This skeletal sternal depression is then divided by the transverse diameter of the vertebral body at that level .
The correction index (CI) requires drawing a horizontal line across the anterior spine. Then two distances are measured: the minimum distance between the posterior sternum and the anterior spine as is used for the HI and the maximum distance between the line placed on the anterior spine and the inner margin of the most anterior portion of the chest. The difference between the two lines is simply the amount of defect the patient has in their chest. If this difference between the measurements is then divided by the maximum prominence of the chest (the longer measurement) and multiplied by 100, it generates the percentage of chest depth the patient is missing centrally. Conversely, it represents the percentage of chest depth to be corrected by bar placement, or the correction index .
The sternal torsion angle is an essential morphologic criterion to note for each patient with pectus excavatum. This is measured in the axial plane by taking the angle of the axis of the mediolateral length to the horizontal. Torsion measured at an angle more than 30° is considered severe, whereas mild torsion is applied to any angle less than 30° .
Treatment and prognosis
Although historically most cases were not treated, and early research suggested that even in extreme cases repair does not offer a significant improvement in respiratory function tests more recently symptomatic improvements in ventilation and perfusion scans, as well as numerous other symptoms, have been described . Importantly, and contrary to earlier beliefs, pectus deformities often persist into adulthood and symptoms may become more pronounced .
In addition to symptoms, the negative effects on body image and normal psychological development should also not be underestimated .
Surgical options include metal bar insertion, rib osteotomies, disconnection of the sternum from costal cartilages and even reversal of the sternum . The Nuss procedure is a minimally invasive procedure where a concave bar is inserted substernally. It has largely replaced the Ravitch procedure which was significantly more invasive.
Differential diagnosis
For the unwary, pectus excavatum can be troublesome on frontal chest radiographs. Differentials include:
- right middle lobe consolidation/atelectasis
- left para-aortic soft tissue density
- lung or paravertebral mass
- atelectasis/consolidation of the medial segment of the left lower lobe
- mediastinal mass due to deformation of the cardiomediastinal contour
The diagnosis is obvious on lateral projection, and of course cross-sectional imaging.
Siehe auch:
- Anomalien des Sternums
- Pectus carinatum
- right middle lobe consolidation
- Haller-Index
- Medial breast margin sign
- Harrenstein-Deformität
- Operation nach Nuss
- cardiomediastinal contour
- chest wall deformity
und weiter:
- Mittellappenatelektase
- Gorlin-Goltz-Syndrom
- radiologisches muskuloskelettales Curriculum
- Nuss procedure
- Noonan-Syndrom
- Fetales Alkoholsyndrom
- occipital horn syndrome
- Ravitch procedure
- x-linked cutis laxa
- differential of an enlarged pulmonary trunk on chest radiography
- Dzierzynsky-Syndrom
- erweiterte Pulmonalarterie
- pectus recurvatum
- Brustwanddeformitäten


 Assoziationen und Differentialdiagnosen zu Pectus excavatum:
Assoziationen und Differentialdiagnosen zu Pectus excavatum:



