septic pulmonary emboli















Septic pulmonary emboli refer to the embolization of infectious particles (intravascular thrombus containing microorganisms) into the lungs via the pulmonary arterial system.
Clinical presentation
Symptoms can be not specific but most manifest as a bacteremia with, dyspnea, chest pain, cough and other respiratory symptoms. Often concurrent symptoms of the extrapulmonary primary infective focus are also present.
Pathology
Septic emboli can originate from different sources :
- right-sided infective endocarditis, particularly tricuspid valve (occasionally pulmonary valve )
- infection elsewhere in the body (e.g. soft tissue infection) with associated septal defects
- infected deep venous thrombosis
- immunological deficiencies
- infected catheters/lines
- venous lines / central venous catheters
- pacemaker wires
- post-anginal septicemia
- periodontal disease
Common pathogens are
- Klebsiella pneumoniae
- Staphylococcus aureus
- Pseudomonas aeruginosa
- Escherichia coli
- Salmonella group B
Radiographic features
The clinical context is significant in image interpretation and differential considerations. Most patients will be clinically septic and have positive blood cultures at the time of imaging assessment.
Plain radiograph
Chest x-ray features are nonspecific but may show :
- peripheral, lower lobe predominant infiltrative densities: can be unilateral or bilateral
- diffuse bilateral nodular densities (often poorly marginated) in varying stages of cavitation
- these nodules generally range between 1-3 cm
- the nodules vary greatly in size, which is a reflection of repeated episodes of embolic shower
- may increase in number or change in appearance (size or degree of cavitation) on subsequent short-term follow up radiographs
- accompanying small pleural effusions can be common
- features suggestive of complicating pleura empyemas may be seen
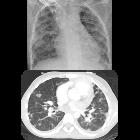
CT
Bilateral abnormalities may be present in as much as 80% of cases .
- feeding vessel sign : peripheral nodules with clearly identifiable feeding vessels associated with lung abscesses
- subpleural nodular lesions or wedge-shaped densities with or without necrosis caused by septic infarcts (these can manifest as cavitary pulmonary infarcts)
- these may have a dependent, lower zone predication
- the wedge-shaped lesions usually range between 10-20 mm
- peripheral nodular densities usually range between 5-35 mm
Treatment and prognosis
Complications
Recognized complications include:
- empyema formation
- pneumothorax formation
Differential diagnosis
For small and/or different size cavitary lung lesions on HRCT or CT chest, consider:
- cavitary pulmonary metastases
- necrobiotic lung nodules
- granulomatosis with polyangiitis (previously known as Wegener granulomatosis)
- pulmonary embolism (thromboembolism)
See also
Siehe auch:
- Lungenarterienembolie
- Granulomatose mit Polyangiitis
- Kavernöse Lungenläsionen
- kavernisierende Lungenmetastasen
- septische Embolie
- necrobiotic lung nodules
- zystische Lungenmetastasen
und weiter:


 Assoziationen und Differentialdiagnosen zu septische Embolie Lunge:
Assoziationen und Differentialdiagnosen zu septische Embolie Lunge:



