temporal lobe epilepsy




Temporal lobe epilepsy (TLE) is the most common type of partial epilepsy, with often characteristic imaging and clinical findings. It is divided into two broad groups:
- most common
- involves the mesial temporal lobe structures
- most frequently due to mesial temporal sclerosis
- involves the inferolateral and lateral neocortex of the temporal lobe
Clinical presentation
Patients with temporal lobe epilepsy demonstrate three phases, each of variable duration and symptomatology:
Pre-ictal phase
A variable number of patients with temporal lobe epilepsy demonstrate or describe an aura, which is usually of short duration, and in most cases (70%) goes on to become a seizure . Auras are variable in symptomatology, and include:
- viscerosensory aura
- typically from lesions of the amygdala or insular cortex
- psychic (experienced) aura
- typically from limbic structures
- variable including dysmnesic phenomena, cognoscitive phenomena, emotional phenomena, delusions, and hallucinations
Ictal phase
The majority of patients have a complex partial seizure, during which a number of relatively specific features may be observed:
- automatisms
- stereotyped motor behaviors, typically of the mouth or hands
- seen in 40-80% of cases
- language alterations
- unilateral dystonic posturing
- versive head turning
Postictal phase
Postictal phase is also variable, and symptoms are largely determined by the location of the ictal lesion. Features include:
- confusion
- drowsiness
- aphasia
- psychiatric symptoms
Pathology
Temporal lobe epilepsy may be due to a veritable menagerie of causes including :
- mesial temporal sclerosis (MTS): ~70%
- temporal lobe tumors: ~10%
- ganglioglioma is the most common
- cortical dysplasia: 5-10%
- vascular malformations: ~5%
- trauma
- infection
- congenital
- temporal pole encephalocele (rare)
Radiographic features
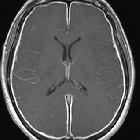
MRI is the modality of choice for structural imaging of the temporal lobe, and of course, appearances will depend on the underlying cause. These are discussed separately, thus please refer to:
- mesial temporal sclerosis
- temporal lobe tumors
- cortical dysplasia
- infection
- vascular malformations
It is essential to review the whole scan carefully as there is a high (5-20%) incidence of dual pathology, especially in cases of cortical dysplasia.
Treatment and prognosis
It is established that chronic medication-resistant epilepsy developed during childhood is linked to cognitive compromise and thus an early aggressive treatment and seizure control is advised for infants and young children .
Treatment depends on the etiology, but in most cases is primarily with antiepileptic medications. In refractory cases, especially when a causative lesion can be identified, temporal lobectomy can be effective, provided cases are carefully selected.
Siehe auch:
- Arteriovenöse Malformation
- Gangliogliom
- Kavernom
- Meningitis
- Hippocampussklerose
- Herpesenzephalitis
- mesial temporal lobe
- kongenitale vaskuläre Malformationen
- Temporallappen
- Tumoren des Temporallappens
und weiter:


 Assoziationen und Differentialdiagnosen zu Temporallappenepilepsie:
Assoziationen und Differentialdiagnosen zu Temporallappenepilepsie: