Zystische Adventitiadegeneration























Cystic adventitial disease (CAD) is an uncommon vascular pathology predominantly affecting peripheral vessels. The vast majority of cases occur in arteries, with venous involvement being an extremely rare occurrence .
Epidemiology
It typically affects young to middle-aged individuals without evidence of atherosclerosis or other systemic vascular disease. There is a recognized male predilection with a M:F ratio of ~15:1 .
Clinical presentation
Although cystic adventitial disease can affect any peripheral vessel, there is a striking predilection in the popliteal region, affected in ~85% of cases .
Typical symptoms include:
- rapidly progressive calf claudication
- lower extremity pain
Pathology
The condition is characterized by a collection of mucinous material (mucous cysts) within adventitial wall of the affected vessel.
Radiographic features
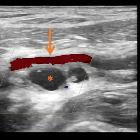
Ultrasound
May show multiple anechoic to hypoechoic lesions within the affected arterial wall. Color Doppler interrogation shows no flow within the lesions. There may also be associated arterial stenoses, with relevant changes in arterial Doppler wave flow and velocity.
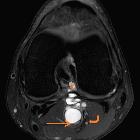
MRI
Appearances on MRI are variable, depending on the distribution and size of the cysts.
May be seen as aggregates of multiple small round/ovoid masses originating in affected arterial wall, which if concentric lead to hourglass stenosis. When the lesions are large, they can have a multi-loculated appearance, and can displace the artery to one side - the so-called scimitar sign .
Lesional signal characteristics include
- T1: individual lesions are of variable signal dependent on mucoid content
- T2/STIR: individual lesions are high signal
Angiography (DSA)
Angiography may demonstrate curvilinear/spiral narrowing of vessels with a paucity of collaterals and an absence of poststenotic dilatation. When cystic lesions are large and eccentric they may displace the artery to one side - the so-called scimitar sign .
History and etymology
It was first described by H J Atkins and J A Key in 1947 .
Differential diagnosis
If in the classical popliteal location on angiography consider popliteal artery entrapment syndrome (PAES).
Siehe auch:
- Aneurysma der Arteria poplitea
- Dissektion
- Arteria-Poplitea-Kompressionssyndrom
- Scimitar-Zeichen
- Zystische Medianekrose Erdheim-Gsell
- Scimitar-Zeichen bei zystischer Adventitiadegeneration
und weiter:


 Assoziationen und Differentialdiagnosen zu Zystische Adventitiadegeneration:
Assoziationen und Differentialdiagnosen zu Zystische Adventitiadegeneration:



