Angiofibrom

Endobronchial
angiofibroma in the aberrant tracheal bronchus presenting as spontaneous pneumomediastinum. a Initial chest X ray shows pneumomediastinum. b Bronchoscopy finding of a protruding and glistering tumour originating from the right side of the trachea. c Computed tomography showing an elongated endobronchial tumour in the accessory tracheal bronchus originating from the right side of the lower tracheal wall (black arrow, axial view). d Computed tomography showing a tumour located in the right upper lobe from the accessory tracheal bronchus (white arrow, coronal view)
Teenager with
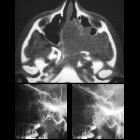
epistaxisAxial CT without contrast of the face (above) shows a large left sided sinonasal soft tissue mass. Early (below left) and later (below right) lateral images from a carotid angiogram show the mass to be hypervascular.The diagnosis was juvenile nasopharyngeal angiofibroma.

Radiofrequency-induced
thermotherapy of nasopharyngeal angiofibroma and immunohistochemical analysis of vessel proliferation: a case report. Scans of a nasopharyngeal angiofibroma. (A) Digital subtraction angiography (maximum intensity projection technique): the terminal branch of the left maxillary artery is at the hilus of the pathological angiofibroma neovascularization. (B) Computed tomography of the viscerocranium: nasopharyngeal angiofibroma seen with intravenous contrast. (C) The same tumor seen with computed tomography carotidography (volume rendering technique).

Multidisciplinary
management of juvenile nasopharyngeal angiofibroma. A Male child, 14 years, presented with epistaxis and nasal obstruction. Nasal biobsy was tried with horrible bleeding CT and MRI showed the presence of nasopharyngeal angiofibroma. Endovascular embolization was done with successful obliteration of tumor blush followed by successful surgical excision. A, B CT PNS (axial and Coronal) shows tumor, C MRI PNS (sagittal T2) shows tumor extensions D, E Distal ECA angiogram lateral view (arterial, and capillary, phases) shows tumor feeders and blush. F Super-selective catheterization of different feeders in different tumor compartments (mainly sphenopalatine artery branches) I–H Control ECA angiogram lateral view (arterial, capillary, and venous phases) shows obliteration of tumor blush in different tumor compartments

Multidisciplinary
management of juvenile nasopharyngeal angiofibroma. A Male child, 13 years, presented with epistaxis and nasal obstruction. CT and MRI showed the presence of nasopharyngeal angiofibroma. Endovascular embolization was done with successful obliteration of tumor blush followed by successful surgical excision. A–C Enhanced MRI PNS (axial, coronal and sagittal) shows tumor extensions D, E CCA angiogram lateral view (arterial, and capillary) shows tumor feeders and blush. F, G Selective and super-selective catheterization of ECA artery (main feeder) H Control ECA angiogram lateral view shows obliteration of tumor blush in different tumor compartments. I–K Control CCA angiogram lateral view (arterial, capillary, and venous phases) shows obliteration of tumor blush in different tumor compartments, L Different parts of totally endoscopic removed tumor

Multidisciplinary
management of juvenile nasopharyngeal angiofibroma. A Male child, 10 years, presented with epistaxis. CT showed the presence of nasopharyngeal angiofibroma. Endovascular embolization was done with successful obliteration of tumor blush followed by successful surgical excision. A–C Enhanced CT scan PNS (axial, coronal and sagittal) shows tumor extensions D–F CCA angiogram lateral view (arterial, capillary, and venous phases) shows tumor feeders and blush. G–I Control CCA angiogram lateral view (arterial, capillary, and venous phases) shows subtotal obliteration of tumor blush in different tumor compartments (except part supplied by ICA)
Angiofibrom
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Angiofibrom:
Assoziationen und Differentialdiagnosen zu Angiofibrom: