Juveniles Angiofibrom

















Juvenile nasopharyngeal angiofibromas are a rare benign, but locally aggressive, vascular tumors that occur almost exclusively in young men.
On imaging, they present as a vividly enhancing soft-tissue masses centered on the sphenopalatine foramen. Given its vascularity, prominent flow voids are seen on MRI leading to a salt and pepper appearance.
Epidemiology
Juvenile nasopharyngeal angiofibromas occur almost exclusively in males and usually in adolescence (~15 years). They account for only 0.5% of all head and neck tumors but are the most common of the benign nasopharyngeal neoplasms.
Clinical presentation
The presentation is typical with obstructive symptoms, epistaxis, and chronic otomastoiditis due to obstruction of the Eustachian tube. Patients may present with life-threatening epistaxis. On examination, it may be seen as a pale reddish-blue mass. It is, as the name suggests, very vascular and a biopsy can sometimes be fatal.
Pathology
Juvenile nasopharyngeal angiofibromas are benign but highly vascular tumors. They may be locally aggressive.
The exact site of origin is contentious as these masses usually present when they have reached a considerable size. However, most authors agree that they arise from the posterior choanal tissues in the region of the sphenopalatine foramen.
Staging
See staging of juvenile nasopharyngeal angiofibromas.
Radiographic features
Imaging plays an important role in diagnosis due to its vascular nature, as biopsies should be avoided due to the risk of brisk hemorrhage, as well as staging.
Although these masses are thought to arise from the region of the sphenopalatine foramen, they are usually sizable at diagnosis, frequently with extension medially into the nasopharynx, laterally into the pterygopalatine fossa and, over time, beyond into the orbit, paranasal sinuses, intracranial cavity and infratemporal fossa.
Plain radiograph
Plain radiographs no longer play a role in the workup of a suspected juvenile nasopharyngeal angiofibroma, however, they may still be obtained in some instances during the assessment of nasal obstruction, or symptoms of sinus obstructions. Findings include :
- visualization of a nasopharyngeal mass
- opacification of the sphenoid sinus
- anterior bowing of the posterior wall of the maxillary antrum (Holman-Miller sign)
- widening of the pterygomaxillary fissure and pterygopalatine fossa
- erosion of the medial pterygoid plate
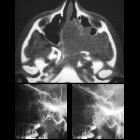
CT
CT is particularly useful at delineating bony changes. Findings are similar to those described above. Typically a lobulated non-encapsulated soft tissue mass is demonstrated centered on the sphenopalatine foramen (which is often widened) and usually bowing the posterior wall of the maxillary antrum anteriorly. There is marked contrast enhancement following administration of contrast, reflecting the prominent vascularity.
Extensive bony destruction is usually not a feature, but rather bone is remodeled or resorbed. This feature may be helpful in differentiating from other more aggressive lesions. An intracranial extension can however occur.
Angiography (DSA)
Angiography, although not essential, is often useful in both defining the feeding vessels as well as in preoperative embolization. Supply of these tumors is usually via :
- external carotid artery: the majority
- internal maxillary artery
- ascending pharyngeal artery
- palatine arteries
- internal carotid artery: less common, usually in larger tumors
- sphenoidal branches
- ophthalmic artery
Of note, enlargement of feeding vessels is not a common finding .
MRI
MRI is excellent at evaluating tumor extension into the orbit and intracranial compartments.
- T1: intermediate signal
- T2: heterogeneous signal: flow voids appear dark
- T1 C+ (Gd): shows prominent enhancement
The presence of prominent flow voids leads to a salt and pepper appearance on most sequences and are characteristic .
Treatment and prognosis
Surgical resection (either open or increasingly endoscopic) is the treatment of choice, usually performed after pre-operative embolization to help with hemostasis. The embolization may be performed up to five days before. Irradiation may be an option if surgery is not possible or only incomplete resection achieved .
In cases where there is skull base involvement, a high recurrence rate (up to 50%) has been reported .
Differential diagnosis
Imaging differential considerations include:
- angiomatous polyp: variant of a sinonasal polyp, located toward ostium/hardly extend to the nasopharynx, elderly age, less vascularity
- rhabdomyosarcoma (head and neck)
- nasopharyngeal carcinoma (NPC)
- nasopharyngeal teratoma
- nasopharyngeal lymphoma
- lymphangioma: no contrast enhancement
- encephalocele: no contrast enhancement
- esthesioneuroblastoma
Siehe auch:
- Tornwaldt-Zyste
- Ästhesioneuroblastom
- Rhabdomyosarkom der Kopf-Hals-Region
- Nasopharynxkarzinom
- Meningoenzephalozele
- Fossa navicularis magna
- Tumoren des Nasopharynx
- Angiofibrom
- Verkalkungen Nasopharynx
- Teratom des Pharynx
- nasales chondromesenchymales Hamartom
- staging of juvenile nasopharyngeal angiofibromas
und weiter:


 Assoziationen und Differentialdiagnosen zu Juveniles Angiofibrom:
Assoziationen und Differentialdiagnosen zu Juveniles Angiofibrom:







