gallbladder perforation





















Gallbladder perforations are a serious complication of acute cholecystitis and represent an advanced stage of the disease. They tend to occur in an elderly and/or comorbid demographic and carry higher rates of morbidity and mortality.
Clinical presentation
Symptoms and clinical signs are variable and can range from benign non-specific abdominal symptoms to acute generalized peritonitis.
The presentation of gallbladder perforation can be indistinguishable from uncomplicated acute cholecystitis .
Pathology
Gallbladder perforation is the result of acute cholecystitis. The sequence of events leading to perforation begin with occlusion of the cystic duct (most often by a calculus), with resultant retention of intraluminal secretions. Distension of the gallbladder with a consequent rise in intraluminal pressure can impede venous and lymphatic drainage, leading to vascular compromise and ultimately to necrosis and perforation of the gallbladder wall.
Regarding the timing of onset, perforation can between two days to several weeks after the onset of acute cholecystitis.
Perforation often occurs iatrogenically during laparoscopic cholecystectomy, with an incidence of estimated to be 15-30% . It can also rarely occur from blunt or penetrating trauma.
Classification
According to the Niemeier classification, there are three main clinical subtypes . A fourth type has been suggested by Andersen et al. .
- type I: acute free perforation
- type II: subacute pericholecystic abscess
- type III: chronic cholecystoenteric fistulation
- type IV: cholecystobiliary fistula formation
Radiographic features
Ultrasound
Ultrasound is the initial investigation of choice. Reported findings include pericholecystic fluid collection(s) with layering of the gallbladder wall .
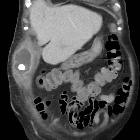
CT
CT is often superior to ultrasound for diagnosis of complications of acute cholecystitis.
Superimposed on background cholecystitis, CT may show:
- defect or bulge in the gallbladder wall
- focal bulge may suggest an occult defect
- pericholecystic fluid collection - evidence of bile leakage
- stranding of the omentum or mesentery
- +/- layering of the gallbladder wall
Treatment and prognosis
Gallbladder perforation may be initially treated by percutaneous cholecystostomy. Patients typically require intravenous antibiotics, volume resuscitation, and close monitoring in an intensive care unit. Eventually (if possible), cholecystectomy is performed .
Given that gallbladder perforation represents an advanced stage of acute cholecystitis, typically occurring in otherwise comorbid patients, the prognosis is often worse. Although very high mortality rates of ~40% were initially reported in the 1940s, contemporary literature cites a mortality rate between 12-16% .
Complications
Reported complications include :
- bile peritonitis
- hepatic abscess formation (possible mechanisms include a direct extension, subcapsular extension and/or haematogenous dissemination via the portal vein)
- subhepatic abscess formation
- pelvic abscess formation
- pneumonia
- pancreatitis
- acute renal failure
Siehe auch:
- perforierte Cholezystitis
- Gallensteinileus
- Bouveret-Syndrom
- akute Cholezystitis
- emphysematöse Cholezystitis
- Cholezystoduodenale Fistel
- cholezystobiliäre Fistel
- hämorrhagische Gallenblasenperforation spontan oder traumatisch
und weiter:


 Assoziationen und Differentialdiagnosen zu Gallenblasenperforation:
Assoziationen und Differentialdiagnosen zu Gallenblasenperforation:




