accessory navicular bone

























An accessory navicular is a large accessory ossicle that can be present adjacent to the medial side of the navicular bone. The tibialis posterior tendon often inserts with a broad attachment into the ossicle. Most cases are asymptomatic but in a small proportion it may cause painful tendinosis due to traction between the ossicle and the navicular. Such changes are best seen on MRI.
Epidemiology
- an accessory navicular bone is present in ~10% (range 4-21%) of the population
- first appears in adolescence
- more common in female patients
- reported bilateral prevalence is ~70% (range 50-90%)
Clinical presentation
Most of the time it is asymptomatic and found incidentally on radiographs, although medial side foot pain (os naviculare syndrome) is the most common presenting feature of accessory navicular bone. The pain is aggravated by walking, running and weight-bearing activities. When large, it can protrude medially and cause friction against footwear.
Gross anatomy
An accessory navicular bone is located posterior to the posteromedial tuberosity of the tarsal navicular bone.
Classification
This classification was proposed by Geist in 1914 and at the time of writing (July 2016) remains the most widely used classification system.
The Geist classification divides these into three types:
- 2-3 mm sesamoid bone embedded within the distal portion of the posterior tibial tendon
- no cartilaginous connection to the naviculam tuberosity and may be separated from it by up to 5 mm
- accounts for 30% of accessory navicular bones
- usually asymptomatic
- accounts for ~55% (range 50-60%) of all accessory navicular bones
- triangular or heart-shaped
- typically measures around 12 mm
- connected to the navicular tuberosity by a 1-2 mm thick layer of either fibrocartilage or hyaline cartilage
- eventual osseous fusion to the navicular tuberosity may take place
- an especially prominent navicular tuberosity called a cornuate navicular
- thought to represent a fused type 2 and is occasionally symptomatic as a result of painful bunion formation over the bony protuberance
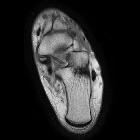
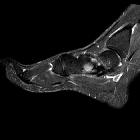
Radiographic features
Radiographs show a medial navicular eminence that is best visualized on the lateral-oblique view. Symptomatic accessory navicular bones may appear as a 'hot spot' on bone scan and on MRI bone marrow edema can be seen.
Treatment and prognosis
Acute pain can be managed can be achieved by corticosteroid injection and immobilization of the foot for 2-3 weeks. For refractory cases, surgical management can be considered.
History and etymology
It is thought to have been first described by Bauhin in 1605 .
See also
Siehe auch:
- akzessorische Knochen Fuß
- Os supranaviculare
- Os naviculare cornutum
- Geist Klassifikation Os tibiale externum
- Morbus Köhler I
- Ossikel
- Os naviculare pedis
- Musculus tibialis posterior
- Lawson-Klassifikation
und weiter:


 Assoziationen und Differentialdiagnosen zu Os tibiale externum:
Assoziationen und Differentialdiagnosen zu Os tibiale externum: