akuter Beckenschmerz in der Schwangerschaft

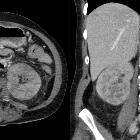
Imaging for
acute pelvic pain in pregnancy. A 27-year-old woman presenting at the emergency department with acute pelvic pain. Abdominal US (a) shows a rounded lesion adjacent to the uterus, clearly separate from the left ovary. Axial CT scan shows a voluminous mass in the pelvic cavity (b); for the characterisation an MRI was required. Axial (c) and coronal (d) T2-weighted and T1-weighted images (e) of the pelvis show a right heterogeneous adnexal mass (arrow) with fallopian tube haematoma. Note the normal ovary (short arrow) in (c). Pre-contrast T1-weighted fat-saturated image (f) shows bloody ascites (short arrows). These findings are due to ectopic pregnancy with tubal rupture and haemoperitoneum

Imaging for
acute pelvic pain in pregnancy. A 35-year-old woman presented with amenorrhea for 7 weeks, abdominal pain and vaginal bleeding; the B-HCG level was elevated. Transvaginal 3D sonogram in sagittal scan shows the interstitial portion of the tube (arrow) located between the gestational sac (GS) and endometrium (e). CT of the pelvis (b) shows a small lesion on the left side of the uterus. Axial (c) and coronal (d) T2-weighted images and axial contrast T1-weighted image (e) of the pelvis show a left gestational-like structure measuring 10 mm in diameter, surrounded by a thick wall according to interstitial pregnancy

Imaging for
acute pelvic pain in pregnancy. A 25-year-old woman at 28 weeks’ gestation with acute pelvic pain and vaginal bleeding. Coronal T2-weighted image (a) shows the intrauterine clot with hypointense areas placed along the right side of the uterine cavity and extended inferiorly to cover the uterine ostium. Coronal T1-weighted fat-saturated gradient-echo image shows the hyperintense subchorionic haematoma (b). Note the normal placenta located on the left side (short arrow)

Imaging for
acute pelvic pain in pregnancy. Coronal (a) and axial (b) T2 HASTE sequences show multiple irregular areas of the placenta bulging into the myometrium with massive invasion of the left parametrium (arrow). These findings are indicative of placenta percreta. An hysterectomy was performed at delivery, which confirmed the presence of placenta percreta

Imaging for
acute pelvic pain in pregnancy. A 38-year-old woman was admitted at 26 weeks’ gestation presenting with vomiting and acute abdominal pain. Axial T2-weighted HASTE (a) and T1-weighted fat-saturated sequences (b) show posterior extravasation of amniotic fluid into a hernial sac that contains a small fluid level; these findings are suggestive of a sealed uterine rupture. Note the presence of haemoperitoneum

Imaging for
acute pelvic pain in pregnancy. Coronal (a) and sagittal (b) T2-weighted MR images show a complex mass, with fluid and solid components on the left ovary. Haemorrhagic areas are seen on T1-weighted sequence (c). Sagittal DWI image shows reduction of diffusion in relationship to the high cellularity of the solid component of the mass (d). Cystoadenocarcinoma was confirmed at surgery

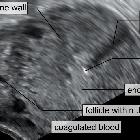
Imaging for
acute pelvic pain in pregnancy. Ovarian torsion in a 38-year-old woman at gestation week 26 with acute pelvic pain. Axial (a), coronal (b) and sagittal (c) T2-weighted sequences show an enlarged, oedematous right ovary (arrow). Axial T1-weighted VIBE fat-saturated sequence (d) shows areas of hypersignal in the context of the right ovary indicative of haemorrhagic infarction

Imaging for
acute pelvic pain in pregnancy. A 33-year-old woman at 32-gestation week was admitted manifesting fever and acute pelvic pain. Coronal diffusion-weighted (DW) image (a) and ADC map (b) show a focal area of restricted diffusion at the level of the upper pole of the left kidney, not seen at T2 Haste (c). The findings are indicative of focal pyelonephritis

Imaging for
acute pelvic pain in pregnancy. Acute appendicitis in a 27-year-old woman at 34-week gestation presenting with abdominal pain on the right side. Coronal (a) T2 image shows a thickened fluid-filled appendix (arrow). Coronal and sagittal T2–weighted HASTE fat-saturated images (b, c) with high signal intensity of periappendicular fat due to inflammatory changes. At surgery and pathology, the diagnosis of appendicitis was confirmed

Imaging for
acute pelvic pain in pregnancy. A 35-year-old woman presents with pubic pain, fever and elevated inflammatory markers. Coronal T2–weighted HASTE image (a) and T2–weighted STIR image (b) show fluid collection (arrow) at the level of the symphisis pubic bone with hyperintensity of the pubic bone (short arrow). Contrast T1-weighted image shows the presence of a thick vascularised wall indicative of an abscess with a small abscess at the level of left pubic bone (short arrow). These findings are in agreement with osteomyelitis


 Assoziationen und Differentialdiagnosen zu akuter Beckenschmerz in der Schwangerschaft:
Assoziationen und Differentialdiagnosen zu akuter Beckenschmerz in der Schwangerschaft: