Binswanger's disease
Subcortical arteriosclerotic encephalopathy (SAE), also known as Binswanger disease or small vessel dementia, refers to slowly progressive exclusively white-matter multi-infarct dementia.
A genetically transmitted form of the disease is known as familial arteriopathic leukoencephalopathy or CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) .
Clinical presentation
Patients usually present with subcortical dementia symptoms including forgetfulness, personality and emotional changes.
Clinical criteria for the diagnosis are as follows:
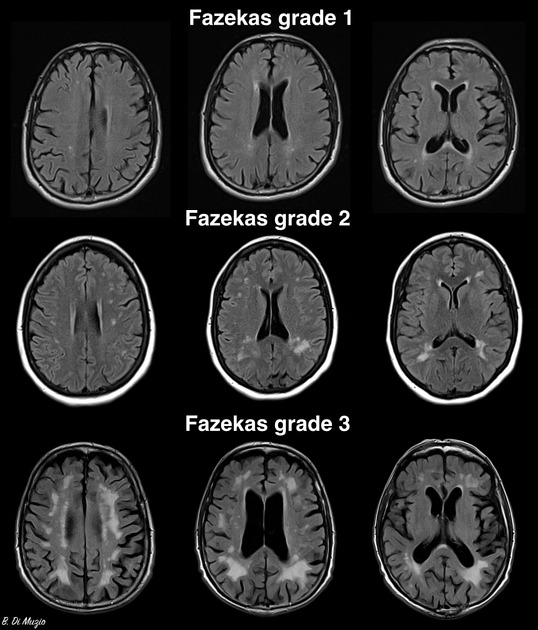
- marked subcortical microangiopathic lesions at MR imaging
- a negative family history for strokes, early cognitive impairment, or psychiatric disorders in first- and second-degree relatives
- documented arterial hypertension: systolic values higher than 160 mm Hg, diastolic values higher than 95 mm Hg, or both, measured on several occasions
Pathology
Pathologically, relatively symmetrical and diffuse bilateral deep periventricular white matter lesions are associated with severe arteriosclerosis of the small penetrating arteries which are thickened, lipohyalinised, stenotic, or even occluded. In most patients, multiple lacunar infarcts are also present in the basal ganglia, thalami, and pons .
Radiographic features
CT
Diffuse, incompletely symmetrical hypodensities are present in deep white matter, especially prominent in the frontal lobes and centrum semiovale .
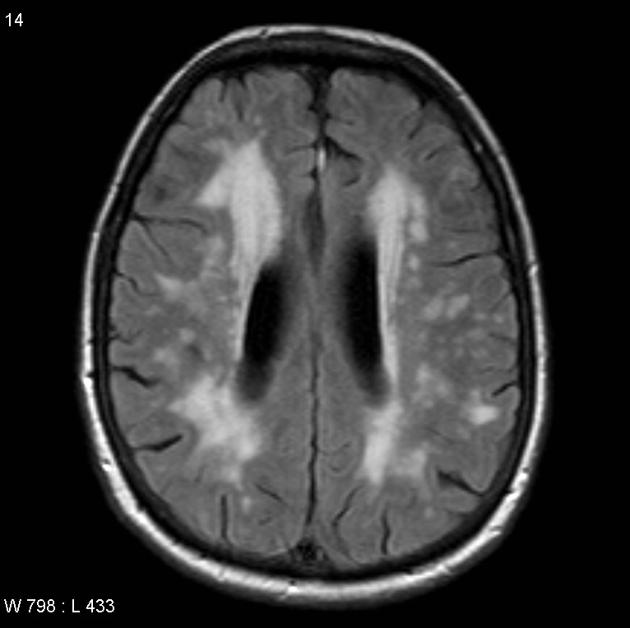
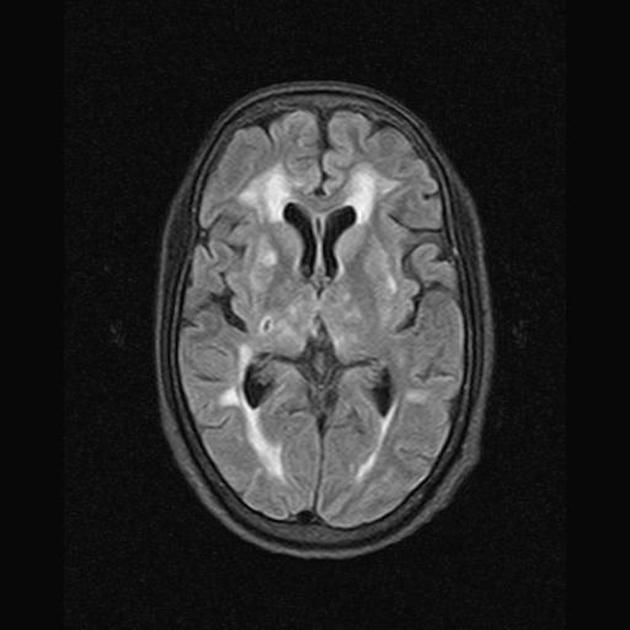
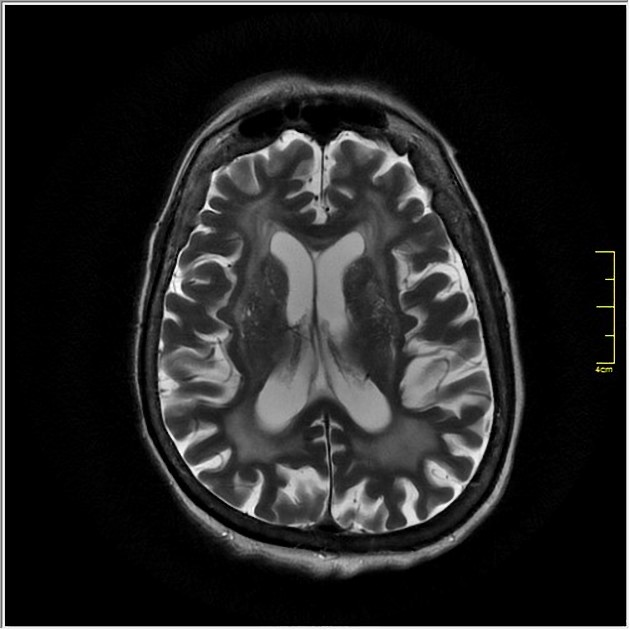
MRI
MRI changes are much more striking, consisting of subcortical and periventricular hyperintense lesions visible on FLAIR, T2-weighted, and proton-density sequences.
The white matter lesions are usually small, commonly grouped around the frontal and occipital horns and in the centrum semiovale.
Moderate diffuse cerebral atrophy is invariably present, and lacunar infarcts in the basal ganglia and thalami are common .
History and etymology
It was first described in 1894 by Otto Ludwig Binswanger (1852-1929), a Swiss psychiatrist and neurologist .
Differential diagnosis
- CADASIL: classically, lesions involve anterior temporal and superior frontal lobes which are uncommonly involved in SAE. Also, arcuate fibers are more likely to be affected in CADASIL. Low signal intensity of the basal ganglia and dentate nuclei of the cerebellum are more pronounced in CADASIL than in SAE .
- CNS vasculitis
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu subcortical arteriosclerotic encephalopathy (SAE):
Assoziationen und Differentialdiagnosen zu subcortical arteriosclerotic encephalopathy (SAE):