Dysplasie der Trochlea femoris






Trochlear dysplasia refers to a dysplastic deformity of the femoral trochlea and is a known risk factor for patellofemoral instability.
Epidemiology
The reported prevalence of trochlear dysplasia in recurrent patellar dislocations is up to 85% . The latter is most common in the adolescent age group .
Clinical presentation
Patients usually present with recurrent lateral patellar dislocation and patellofemoral instability.
Pathology
Dysplastic deformity of the distal anterior femoral surface, precisely of the most superior aspect of the trochlea in a way, that it poses a predisposition factor for the patella to dislocate during the transition from the fully extended status of the knee to the early knee flexion.
Radiographic features
Different radiographic methods exist to assess for trochlear dysplasia in true lateral radiographic images of the knee and cross-sectional imaging CT and MRI respectively.
Classification of trochlear dysplasia as described by Dejour
- type A: crossing sign, normal facet geometry but shallow trochlea
- type B: crossing sign, trochlear spur on lateral radiograph and flat trochlear groove on cross-sectional imaging
- type C: crossing sign and double contour on lateral radiograph with medial facet hypoplasia and lateral facet convexity
- type D: crossing sign, trochlear spur and double contour on the lateral radiograph and a cliff-like pattern between the medial and lateral facets
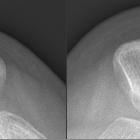
Plain radiograph
Initial evaluation based on a true lateral knee radiograph :
- crossing sign: the intersection of the trochlear floor and lateral femoral condyle contours
- supratrochlear spur: bony spur at the most proximal portion of the trochlea
- double contour sign: significantly smaller medial femoral condyle
- trochlear bump: the increased distance between the anterior trochlear groove and extension of the anterior cortex of the distal femur
- sulcus angle
MRI
Different methods for the assessment exist :
Lateral trochlear inclination (LTI)
- inclination angle between the lateral trochlear facet and a posterior condylar tangential line
- evaluation on the most cranial/ proximal axial slice containing trochlear cartilage
- an angle <11° indicates trochlear dysplasia (reported sensitivity and specificity: 93%/87%)
Trochlear depth (TD)
- different methods with different normal values exist also depending on whether bony or cartilaginous contours are used
- a simple method is to measure the distance between the floor of the trochlear and a tangential line connecting the most anterior points of the medial and lateral facet
- a trochlear depth <3 mm indicates trochlear dysplasia
Ventral trochlear prominence
- distance between the anterior cortex of the distal femur and the most anterior cartilaginous point of the trochlear groove on a sagittal plane through the trochlear groove
- a distance >8 mm indicates trochlear dysplasia (sensitivity and specificity: 75%/83%)
Medial condyle trochlear offset (MCTO)
measured as the distance between the medial condyle and a tangential line through the trochlear groove parallel to the posterior sufaces of the femoral condyles
Facet asymmetry (FA)
- the ratio between medial versus lateral trochlear facet length calculated as (medial facet) / (lateral facet) is one way to calculate it
- a ratio of <40%, in this case, indicates trochlear dysplasia
Radiology report
There is a poor correlation between the classical and still commonly used Dejour classification system and the measurements derived from axial MR images. This should be taken into account when indicating trochlear dysplasia. The radiological report should, therefore, contain a qualitative description as well as the metric used for the diagnosis of trochlear dysplasia.
Treatment and prognosis
Trochlear dysplasia is a predisposing factor of patellofemoral instability and should be only treated in that context.
The treatment of high-grade trochlear dysplasia is trochleoplasty, which aims at correcting the trochlear depth abnormality by recreating a centralized groove, which facilitates the entry of the patella during early knee flexion.
In symptomatic patients with recurrent patellar dislocations and failure of previous patellar alignment surgery or non-operative management or trochleoplasty can be proposed as an indication .
Different surgical techniques of trochleoplasty exist and include :
- sulcus-deepening trochleoplasty
- recession-wedge trochleoplasty
- elevation of the lateral trochlear facet
The clinical outcome seems to depend on the type of dysplasia and seem to show better results after surgical correction of Dejour type B and type D dysplasia.
Practical points
The need for a simplified approach in respect to grading of trochlear dysplasia assessed on MR images has been formulated and a simplified grading into low-grade and high-grade trochlear dysplasia has been proposed . This is also due to a poor correlation with the original Dejour classification system .
Since cross-sectional images and radiographs show different aspects of trochlear dysplasia it might be worthwhile acquiring both if there are doubts with respect to the diagnosis.
A review regarding the quality assessment of radiological measurements identified the following metrics as most useful for the assessment of trochlear dysplasia : the lateral trochlear inclination (LTI), the crossing sign, the trochlear bump, the TT-TG for planning treatment, the trochlear depth and the ventral trochlear prominence.
See also
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Dysplasie der Trochlea femoris:
Assoziationen und Differentialdiagnosen zu Dysplasie der Trochlea femoris: