Ösophagusruptur

Infant with
hematemesis who had an unsuccessful nasogastric tube placementCXR AP shows air outlining the heart in the pericardial space, air outlining the thymus in the mediastinum, and air in the bilateral pleural spaces.The diagnosis was pneumopericardium, pneumomediastinum, and pneumothorax due to esophageal perforation from traumatic nasogastric tube placement. A subsequent esophagram did not demonstrate a leak.

Boerhaave
syndrome – spontaneous oesophageal perforation. Contrast-enhanced CT of the chest showing pneumomediastinum around the oesophagus. A large fluid collection with air fluid level is seen transversing the mediastinum. The fluid collection communicates with both pleural cavities.

Boerhaave
syndrome – spontaneous oesophageal perforation. Contrast-enhanced CT of the chest showing large fluid collections in the pleural cavities. Air is noted in the pleural cavities.

Imaging of
the oesophagus: beyond cancer. Complication of food impaction with tear of oesophagus during chicken bone extraction. a Pre-contrast axial image of the thorax demonstrates a markedly enlarged oesophagus which is high in density (*) when compared to the adjacent blood pool in the aorta (findings consistent with hematoma). b Post-contrast imaging of the same patient demonstrates areas of active contrast extravasation (arrows) within a markedly enlarged and abnormal appearing oesophagus. Clinical note, patient subsequently had multiple episodes of hematemesis
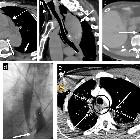
Esophageal
emergencies: another important cause of acute chest pain. Esophageal perforation. a, b Iatrogenic esophageal perforation. Eighty-year-old woman with chest pain after transesophageal echocardiography. Axial (a) and sagittal (b) CT images show a dilated and blood-filled upper esophagus (asterisk) contiguous with a large posterior hematoma containing multiple locules of gas (long arrow). Extensive hemo-pneumomediastinum (dashed arrow), small bilateral pleural effusions (short arrow), and subcutaneous emphysema in the lower neck (arrowhead) are seen. c, d Boerhaave syndrome. Eighty-seven-year-old woman with epigastric and back pain after forceful vomiting. c Axial CT image at the gastroesophageal junction shows extraluminal gas surrounding the lower esophagus (arrow). Bilateral pleural effusions (asterisk). d Single contrast esophagography demonstrates luminal narrowing and irregularity of lower esophagus (arrow) with large contrast extravasation into the left pleural space (asterisk). e Traumatic esophageal perforation. Twenty-five-year-old male with gunshot wound to the chest. Axial CT image shows a bullet tract from right axilla to the left upper hemithorax (dashed arrow) resulting in bilateral pneumothoraces (not shown), left hemothorax (asterisk), and pulmonary contusion and laceration in the bilateral upper lobes (arrow). There is esophageal thickening and indistinctiveness with a small hematoma (circle) representing esophageal injury/perforation

Gastrointestinal
perforation: clinical and MDCT clues for identification of aetiology. 75-year-old patient with oesophageal intramural rupture. a Axial unenhanced image demonstrates blurring of paraoesophageal fat, a double air-filled lumen and an interposed diaphragm (arrow) consistent with a flap. b Axial and (c) sagittal unenhanced images following oral contrast administration demonstrate contrast at the dependent part of the lumen (*) and a submucosal curvilinear collection of gas (arrowhead) better demonstrated on the sagittal plane (open arrow), giving the oesophagus a double-barreled appearance
Ösophagusruptur
Siehe auch:
- Boerhaave-Syndrom
- Ösophagusperforation
- intramurale Dissektion des Ösophagus
- traumatische Ösophagusruptur
und weiter:


 Assoziationen und Differentialdiagnosen zu Ösophagusruptur:
Assoziationen und Differentialdiagnosen zu Ösophagusruptur:

