pilomyxoid astrocytoma


Pilomyxoid astrocytomas are an uncommon and aggressive variant of pilocytic astrocytoma with unique clinical and histopathologic characteristics.
Epidemiology
Pilomyxoid astrocytomas are usually encountered in young children and infants (mean age of 10-18 months), however, adults cases have been described . As most of these tumors have been previously classified as pilocytic astrocytomas it is uncertain whether they have distinctive epidemiology .
Clinical presentation
There is no characteristic clinical presentation and the symptoms will be related to the mass effect and the tumor location . Usually symptoms relating to increased intracranial pressure or parenchymal compression will be present .
Pathology
Grading
Although it has been suggested that pilomyxoid astrocytomas should be considered WHO grade II tumors (compared to pilocytic astrocytomas which are WHO grade I), in the 2016 update to the WHO classification of CNS tumors a formal grade has not been given .
Location
Pilomyxoid astrocytomas were originally reported as arising in the hypothalamus or optic chiasm, which is the most common location, however, they may also occur elsewhere within the brain, including the posterior fossa, as well as in the spinal cord .
Microscopic features
Pilomyxoid astrocytomas are composed of monomorphous bipolar cells with a prominent angiocentric pattern. They are embedded within a profoundly myxoid background . Generally, these tumors are well circumscribed without infiltration .
Features typically found in pilocytic astrocytomas, such as Rosenthal fibers, eosinophilic granular bodies and calcification are uncommon or absent in pilomyxoid astrocytomas . These tumors also lack the biphasic appearance (dense cellular areas alternating with loose cystic areas) usually present in pilocytic astrocytomas .
Vascular proliferation and foci of necrosis are only occasionally encountered .
Immunophenotype
Generally these tumors show astrocytic immunohistochemistry :
- GFAP: positive
- S100: positive
- vimentin: positive
- synaptophysin: variable
- NFP: negative
- chromogranin-A: negative
- BRAF (V600E-mutant): negative
Radiographic features
These tumors are usually large, well-circumscribed, lobulated and may have solid or cystic components with no or minimal surrounding edema. They are typically described as H-shaped as they expand from the midline ( hypothalamic and optic chiasma region )into both temporal lobes. Hemorrhagic components may be present. CSF dissemination can also be seen.
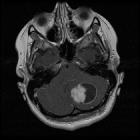
MRI
Reported signal characteristics include:
- T1: isointense
- T2: usually hyperintense, reflecting its myxoid matrix
- GRE/SWI: approximately 20% show intratumoral hemorrhage
- T1 C+ (Gd): common and is usually in the solid component but can be also peripheral
- DWI/ADC: usually high ADC values (facilitated diffusion), reflecting its myxoid matrix
Treatment and prognosis
Compared to pilocytic astrocytomas, pilomyxoid astrocytomas have been generally thought to behave more aggressively and have a poorer prognosis, although this may be in part at least due to their predilection for the hypothalamus and optic chiasm, which makes complete resection impossible .
The total resection of the tumor is the most reliable predictor of a favorable outcome .
Differential diagnosis
Pilocytic astrocytoma is the main differential diagnosis, and no reliable imaging features can distinguish between them, although certain features are more common in pilomyxoid astrocytomas, including:
- hemorrhage
- hypothalamic-chiasmatic involvement
- very young age (<2 years of age)
- H shaped large supra sellar mass
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu pilomyxoides Astrozytom:
Assoziationen und Differentialdiagnosen zu pilomyxoides Astrozytom:
