Post radiation myelitis


Radiation myelitis isa white matter injury of the spinal cord caused by ionizing radiation after a latent period. It is a rare serious complication of radiotherapy and is often a diagnosis of exclusion . It is one of the special forms of myelitis that occurs due to irradiation of a nearby malignancy (e.g. nasopharyngeal carcinoma, vertebral metastasis). Its incidence has much decreased due to confidence in dose prescription and delivery with novel techniques and clinical expertise of spinal cord tolerance.
Terminology
Acute transient radiation myelopathy develops after irradiation of the spinal cord at the end of the first year (6-12 months).
Delayed radiation myelopathy (progressive radiation myelopathy) is a rare but serious complication of radiotherapy. It usually occurs in 9-18 months after completion of radiotherapy.
Clinical presentation
The neurological manifestations are specific to the area affected of the spinal cord.
Pathology
Several factors affect its occurrence and severity, such as radiation dose, fractionation or linear energy transfer. Glial cells and vascular endothelium are proposed to be the main targets affected. Radiation-induced vascular damage results in vascular hyperpermeability and venous exudation . It can occur even within the accepted tolerance limits for the spinal cord .
Radiographic features
PET-CT scans may be used for differential diagnosis of radiation myelopathy from primary spinal cord lesions and spinal metastases .
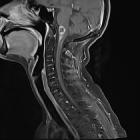
MRI is more sensitive than CT for spinal cord lesions. MRI may be normal in radiation myelopathy. Suggested features are:
- intramedullary hyperintensity on T2 sequences
- marginal/heterogeneous enhancement in T1 postcontrast sequences
- spinal cord edema
- cord expansion
- hemorrhagic changes in severe cases with poor outcome
Central region of spinal cord is more affected as it contains spinal grey matter with myelinated tracts at the periphery.
Treatment and prognosis
As the spinal cord injury is irreversible, treatment is usually supportive. Some patients may benefit from corticosteroids, warfarin, pentoxifylline, vitamin E, and hyperbaric oxygen treatments . Although the damage is presumptively permanent, some patients show neurological improvement and recovery on follow up which may be due to resolution of cord edema and inflammation or possible remyelination and revascularization .
Differential diagnosis
The differential diagnosis includes:
Practical points
To consider such diagnosis, the following criteria should be confirmed :
- the affected spinal cord segment must be in the irradiated zone
- symptoms must correspond to the involved spinal cord segment
- presents after a latency period of more than six months
- absence of spinal cord metastases
- absence of primary spinal cord lesions
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Progressive radiation myelopathy:
Assoziationen und Differentialdiagnosen zu Progressive radiation myelopathy: