vertebral metastases




















Vertebral metastases represent the secondary involvement of the vertebral spine by haematogenously-disseminated metastatic cells. They must be included in any differential diagnosis of a spinal bone lesion in a patient older than 40 years.
This article will focus only on the metastasis involving the bony structures of the spine; please refer to the specific articles for other spinal metastatic diseases:
Epidemiology
Vertebral metastases are already present in 10% of newly-diagnosed cancers. They are much more frequent in higher age groups (>50 years).
Clinical presentation
Vertebral lesions are very frequently asymptomatic in the setting of widespread metastatic disease, and are thus often found incidentally when imaging is performed for other reasons (e.g. staging).
Lesions may become symptomatic due to bone pain, pathological compression fractures, or extension into the spinal canal with cord compression and ensuing neurological deficits.
Pathology
The most common primary malignancies to involve the vertebrae include:
- breast cancer
- lung cancer
- prostate cancer
- lymphoma
- renal cell carcinoma
- gastrointestinal tract malignancies
- melanoma
- pancreatic cancer
- thyroid carcinoma
- carcinoid
Metastases are either osteoblastic or osteolytic, however osteoid formation and mineralization is of limited help in determining the primary tumor as some metastases may secrete osteoblast- and osteoclast-stimulating factors at the same time. New bone formation may also occur after chemotherapy or radiation therapy. Having said that some primaries more frequently result in sclerosis than others.
Primaries with predominantly osteoblastic metastases (sclerotic extradural bone lesions) include:
Primaries with predominantly osteolytic metastases, that may rarely become osteoblastic (mixed sclerotic and lytic extradural bone lesions) include:
Primaries with osteolytic metastases include:
- lung cancer
- gastrointestinal tract cancers
- renal cell carcinoma
- malignant melanoma
- multiple myeloma
Radiographic features
Metastatic lesions can have virtually any appearance. They can mimic a benign lesion or an aggressive primary bone tumor. It can be difficult, if not impossible, to judge the origin of the tumor from the appearance of the metastatic focus, although some appearances are fairly characteristic.
Plain radiograph
Radiographs are useful as an overview but are insensitive to small lytic lesions and struggle to assess for compromise of the canal. As metastases have a predilection for involving the posterior vertebral body and pedicle, a missing pedicle (see: absent pedicle sign) is a useful and subtle sign to seek on AP films.
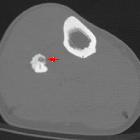
CT
The appearance on CT will depend on the degree of mineralization of the metastasis. The more common lytic metastases appear as regions of soft tissue attenuation with irregular margins. The mass may breach the cortex and result in compromise of the spinal canal.
Sclerotic lesions appear hyperdense and irregular but are less likely to extend beyond the vertebrae.
MRI
MRI is sensitive to metastatic disease and is able also to assess for cord compression. The signal intensity of the metastatic deposits will vary according to the degree of mineralization.
Osteoblastic metastases
- T1: hypointense
- T2: hypointense
Mixed sclerotic and lytic extradural bone lesions
- T1: hypointense
- T2: hypo- and/or hyperintense
Lytic extradural bone lesions
- T1: intermediate to hypointense
- T2: hyper- or isointense
- T1 C+ (Gd): enhancement usually present
Treatment and prognosis
The spinal instability neoplastic score (SINS) can be used to assess for spinal stability in the presence of vertebral metastases. A score of 7-18 warrants surgical consultation.
Differential diagnosis
For osteoblastic metastases consider:
- bone islands (enostoses)
- spondylosclerosis hemispherica
- primary bone tumors (osteoblastoma, osteoid osteoma)
- therapy effects (radiation, chemotherapy, vertebroplasty)
(mostly solitary lesions, patients may however present with a history of cancer)
For mixed sclerotic and lytic extradural bone lesions consider:
- primary bone tumors
- therapy effects
- radiation
- chemotherapy
- vertebroplasty
For lytic extradural bone lesions consider:
- primary bone tumors
- aneurysmal bone cyst
- neurilemmoma/schwannoma
- infective spondylitis
- atypical hemangioma
See also
Siehe auch:
- Myelonkompression
- Hämangiom der Wirbelsäule
- osteoblastische Knochenmetastasen
- Kompaktainsel
- Aneurysmatische Knochenzyste
- Osteoid-Osteom
- Glioblastoma multiforme
- osteolytische Knochenmetastasen
- Oligodendrogliom
- Ependymom
- Multiples Myelom
- Schwannom
- Transverse Myelitis
- Medulloblastom
- Hämangioblastom
- Osteoblastom
- Astrozytom
- spinale Schwannome
- Syringomyelie
- chronisch adhäsive Arachnopathie
- neoplasms of the spinal canal
- spinal neurofibroma
- intradural extramedullary metastases
- intraspinales Meningeom
- Knochenmetastasen
- spinale Metastasen
- Myelopathie durch spinale Enge
- Vertebroplastie
- Tumoren des Plexus choroideus
- intramedullary metastases (spinal)
- Fibröse Dysplasie der Wirbelsäule
- Myelonkompression durch Metastasen
- the winking owl sign
- neurilemmoma
- Metastasen Nierenzellkarzinom Wirbelsäule
- sugar coating
und weiter:
- atypisches Hämangiom Wirbelkörper
- diffus hypointenses Knochenmarksignal in T1
- Platyspondylie
- Vertebra plana
- Aseptische Wirbelkörpernekrose
- Sarkoidose ossäre Manifestationen
- Gibbus
- intramedullary spinal metastasis
- musculoskeletal manifestations of sarcoidosis
- low endplate signal on T1
- lung carcinoma with vertebral metastasis
- absent pedicle sign
- Vorhangzeichen
- Tumoren der Halswirbelsäule
- vertebral metastases: absent pedicle
- Wirbelkörpermetastasen in der Röntgenaufnahme


 Assoziationen und Differentialdiagnosen zu vertebrale Metastasen:
Assoziationen und Differentialdiagnosen zu vertebrale Metastasen: