osteosarcoma




































Osteosarcomas are malignant bone-forming tumors. They are the second most common primary bone tumor after multiple myeloma, accounting for ~20% of all primary bone tumors. They can be classified into primary and secondary forms, as well as histologic types, of which conventional osteosarcoma is the most common.
Epidemiology
Primary osteosarcoma typically occurs in young patients (10-20 years) with 75% taking place before the age of 20 because the growth centers of the bone are more active during puberty/adolescence .There is a slight male predominance.
Secondary osteosarcoma occurs in the elderly, usually secondary to malignant degeneration of Paget disease, extensive bone infarcts, post-radiotherapy for other conditions, osteochondroma, and osteoblastoma.
Associations
- Paget disease of bone
- irradiation
- Rothmund-Thomson syndrome
- fibrous dysplasia (more common in the polyostotic form)
- Mazabraud syndrome (rare)
Clinical presentation
Patients often present with bone pain, occasionally accompanied by a soft-tissue mass or swelling. At times, the first symptoms are related to pathologic fracture.
Pathology
Location
Primary osteosarcomas typically occur at the metadiaphysis of long bones in the appendicular skeleton, most commonly at the following sites:
- femur: ~40% (especially distal femur)
- tibia: ~16% (especially proximal tibia)
- humerus: ~15%
Other sites are less common:
- fibula
- innominate bone (i.e. os coxae)
- mandible (gnathic osteosarcoma)
- maxilla
- vertebrae
Secondary tumors, on the other hand, have a much wider distribution, largely mirroring the combined incidence of their underlying conditions, and thus much have a higher incidence in flat bones, especially the pelvis (a favorite site of Paget disease).
Osteosarcomas can be further categorized by anatomic relationship to the bone:
- intramedullary/central: ~80%
- surface: ~10-15%
- intracortical osteosarcoma: rare
- extraskeletal osteosarcoma: ~5%
Classification
The WHO classification of bone tumors lists the histologic types of osteosarcoma, which can be further organized by the state of underlying bone and site of origin within the bone:
- primary osteosarcoma
- intramedullary/central
- conventional osteosarcoma: most common (75-80%) and discussed in this article
- low-grade central osteosarcoma
- telangiectatic osteosarcoma
- small cell osteosarcoma
- surface
- intramedullary/central
- secondary osteosarcoma
Conventional osteosarcomas can be further divided by histological subtype:
- osteoblastic (most common)
- chondroblastic
- fibroblastic
Macroscopic appearance
Osteosarcomas are bulky tumors where a heterogeneous cut surface demonstrates areas of hemorrhage, fibrosis, and cystic degeneration. Their extension within the medullary cavity is often much more extensive than the bulky part of the tumor would suggest. Areas of bone formation are characteristic of osteosarcomas, with the degree of bone formation varying widely.
Microscopic appearance
Poorly formed trabecular bone is seen with (in the typical high-grade conventional subtype) cellular pleomorphism and mitoses. Variable amounts of fibrocystic and chondroblastic appearing cells may also be encountered.
Markers
Serum alkaline phosphatase (ALP) may be raised (particularly with advanced disease).
Radiographic features
Although plain radiography can provide a lot of information, MRI is used for local staging by assessing intraosseous tumor extension (e.g. growth plate/epiphysis, skip lesions) and soft-tissue involvement. Chest CT and bone scanning have a role in distant staging.
Plain radiograph
Conventional radiography continues to play an important role in diagnosis. Typical appearances of conventional high-grade osteosarcoma include:
- medullary and cortical bone destruction
- wide zone of transition, permeative or moth-eaten appearance
- aggressive periosteal reaction
- sunburst type
- Codman triangle
- lamellated (onion skin) reaction: less frequently seen
- soft-tissue mass
- tumor matrix ossification/calcification
- variable: reflects a combination of the amount of tumor bone production, calcified matrix, and osteoid
- ill-defined "fluffy" or "cloud-like" compared to the rings and arcs of chondroid lesions
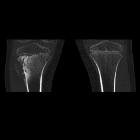
CT
The role of CT is predominantly utilized in assisting biopsy and staging. CT adds little to plain radiography and MRI in the direct assessment of the tumor. The exception to this rule is predominantly lytic lesions in which small amounts of mineralized material may be inapparent on both plain film and MRI .
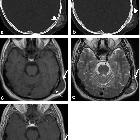
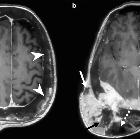
MRI
MRI is proving an essential tool to determine accurate local staging and assessment for limb-sparing resection, particularly for evaluation of intraosseous tumor extension and soft-tissue involvement. Evaluation of the growth plate is also essential as up to 75-88% of metaphyseal tumors do cross the growth plate into the epiphysis .
- T1
- soft tissue non-mineralized component: intermediate signal intensity
- mineralized/ossified components: low signal intensity
- peritumoral edema: intermediate signal intensity
- scattered regions of hemorrhage will have a variable signal (see aging blood on MRI)
- enhancement: solid components enhance
- T2
- soft tissue non-mineralized component: high signal intensity
- mineralized/ossified components: low signal intensity
- peritumoral edema: high signal intensity
Treatment and prognosis
Cure, if achievable, requires aggressive surgical resection often with amputation followed by chemotherapy. If a limb-salvage procedure is feasible, a course of multidrug chemotherapy precedes surgery to downstage the tumor, followed by wide resection of the bone and insertion of an endoprosthesis. The outcome depends on different factors such as age, sex, site, size, and type but the most important predictor is the histologic degree of necrosis post-induction chemotherapy; 90% histologic necrosis is associated with much better prognosis . Currently, the 5-year survival rate after adequate therapy is approximately 60-80% .
The most frequent complications of conventional osteosarcoma are a pathologic fracture and the development of metastatic disease, particularly to bone, lung, and regional lymph nodes.
Differential diagnosis
General differential considerations include the following:
When the lesion is at the posteromedial distal femur, consider
Practical points
When planning to biopsy a potential sarcoma, the treating surgeon should be consulted to plan the biopsy track as this will require excision to reduce the chance of seeding. A poorly planned track that crosses compartments can result in a more extensive resection, potentially with poor outcomes for the patient.
Siehe auch:
- Osteomyelitis
- Aneurysmatische Knochenzyste
- Ewing-Sarkom
- kortikales Desmoid
- parossales Osteosarkom
- Osteosarkom des Femurs
- maligne Entartung fibröse Dysplasie
- Osteosarkom der Tibia
- sarkomatöse Entartung bei Morbus Paget des Knochens
- Osteosarkom bei Erwachsenen
- teleangioektatisches Osteosarkom
und weiter:
- Codman-Dreieck
- Kompaktainsel
- verkalkte Lungenherde
- Osteoid-Osteom
- Osteopoikilose
- Myositis ossificans
- Pierre-Marie-Bamberger-Krankheit
- Weichteilverkalkungen
- Osteom NNH
- Synovialsarkom
- tumoröse Kalzinose
- Tumoren der Nasennebenhöhlen
- Sunburstzeichen
- solide Periostreaktion
- miliare Lungenherde
- clavicle abnormalities (paediatric)
- desmoplastisches Fibrom
- radiologisches muskuloskelettales Curriculum
- Knochentumoren
- differential diagnosis of calcified pulmonary densities
- teleangiektatisches Osteosarkom
- periostales Osteosarkom
- subunguale Exostosen
- osseous lesions preferentially involving the epiphysis
- solitary sclerotic bone lesion
- ivory vertebra sign
- miliary nodules in the exam
- Läsionen des Sakrums
- Rothmund-Thomson syndrome
- maligne Tumoren des Herzen
- differential diagnosis for calcified masses in the mandible
- Knochenläsionen der Epiphyse
- Raumforderungen im oder am Sinus cavernosus
- Sarkom
- primäre maligne Neoplasien des Herzens
- osteosarcoma with sunburst periosteal reaction
- cementifying fibroma
- paediatric clavicle abnormalities
- disorganised periosteal reaction
- Sklerosierung der Klavikula
- malignancies in childhood
- primary tumours of the spine
- bone-forming tumours
- dystrophic soft-tissue calcification
- multiple Osteolysen
- osteoid lesions
- spikulierte Periostreaktion
- Sklerose des Sternoclaviculargelenks
- Lungenmetastasen bei Osteosarkom
- Knochenläsionen der Metaphyse
- Osteosarkom der Patella
- Osteosarkom des distalen Femurs
- lamellenartige Periostreaktion
- osteosarcoma with pathological fracture
- Osteosarkom des Beckens
- Osteosarkom der Rippen
- Osteosarkom Humerus
- Os ilium Osteosarkom
- paediatric bone tumours (differential diagnosis)
- Tumoren der Klavikula
- osteosarcoma - distal tibia
- hyperdense pulmonale Raumforderungen
- teleangectatic osteosarcoma
- Osteosarkom der Fibula
- Osteosarkom des Sternums
- osteosarcoma of the tibia in a child
- Osteosarkom des Larynx
- Osteosarkom Wirbelsäule
- skip lesions in osteosarcoma
- Osteosarkom Fuss
- maxillar osteosarcoma
- osteosarcoma - conventional (histology)
- distribution of osteosarcoma
- knochenbildende Tumoren


 Assoziationen und Differentialdiagnosen zu Osteosarkom:
Assoziationen und Differentialdiagnosen zu Osteosarkom: