testicular microlithiasis





















Testicular microlithiasis is a relatively uncommon condition that represents the deposition of multiple tiny calcifications throughout both testes.
The most common criterion for diagnosis is that of five microcalcifications in one testicle, although definitions have varied in the past. In the majority of cases, testicular microlithiasis is bilateral.
Epidemiology
Testicular microlithiasis is seen in up to 0.6% of patients undergoing scrotal ultrasound. Some reports suggest that it may present in up to 5.6% of the general population between 17 and 35 years of age . Although testicular microlithiasis is present in ~50% of men with a germ cell tumor, it is very common in patients without cancer, and a direct relationship between the two has been debated.
Associations
- testicular germ cell tumor
- Klinefelter syndrome
- cryptorchidism
- testicular infarct
- testicular granulomatous disease
- infertility
- Down syndrome
- alveolar microlithiasis
Clinical presentation
Testicular microlithiasis per se is asymptomatic and is usually found incidentally when the scrotal content is examined with ultrasound, or found in association with symptomatic conditions.
Pathology
The microcalcifications are likely a marker of tubular degeneration, but not a risk factor for tubular degeneration .
Radiographic features
Ultrasound
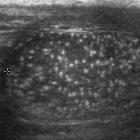
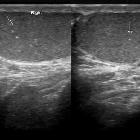
Ultrasound is the modality of choice for examining the testes. Microlithiasis appears as small non-shadowing hyperechoic foci ranging in diameter from 1-3 mm. These foci, often uniformly sized, occur within the testicular parenchyma and although usually distributed uniformly, may be distributed peripherally or segmentally .
One classification scheme used on ultrasound, suggested by ESUR scrotal imaging guidelines is :
- limited TML: less than 5 microcalcifications per field of view
- classic TML: greater than or equal to 5 microcalcifications per field of view
- diffuse TML: numerous microcalcifications
It is unclear if a grading system adds prognostic value, however, relative to follow up based on known risk factors.
Treatment and prognosis
Testicular microlithiasis is in itself asymptomatic and benign. A relationship with testicular tumors, in particular germ cell tumors (GCT) is controversial. An ~12 fold increased risk of GCT in symptomatic testicles with microlithiasis has been reported (with microlithiasis found in approximately 50% of GCT cases), however, no increased risk has been found in asymptomatic testicles. It is also unclear whether early detection confers any benefit over self-exam. As such, screening is unlikely to be beneficial .
Some publications advise routine self-examination rather than sonographic surveillance while others recommend annual ultrasound follow up when it is accompanied by other premalignant factors.
The European Society of Urogenital Radiology (ESUR) advises annual ultrasound follow-up until age 55, only if a risk factor for malignancy is present which include:
- maldescent
- orchidopexy
- testicular atrophy (e.g. volume under 12 cc)
- previous germ cell tumor
- family history of germ cell tumor
Siehe auch:
- Down-Syndrom
- Kryptorchismus
- Skrotolith
- alveoläre Mikrolithiasis
- skrotale Verkalkungen
- testicular germ cell tumour
- Verkalkungen des Hodens
- Merkspruch Keimzelltumoren
und weiter:


 Assoziationen und Differentialdiagnosen zu Mikrolithiasis testis:
Assoziationen und Differentialdiagnosen zu Mikrolithiasis testis:


