Tracheomalazie






 nicht verwechseln mit: Säbelscheidentrachea
nicht verwechseln mit: SäbelscheidentracheaTracheomalacia, or sometimes described as tracheobronchomalacia, is a common incidental finding on imaging of the chest of older patients and manifests as an increase in tracheal diameter as well as a tendency to collapse on expiration.
Tracheomalacia can be broadly considered as being congenital or acquired. The remainder of this article relates to acquired tracheomalacia, while a separate article considers the specifics of congenital tracheomalacia.
Terminology
There are overlap and inconsistency in the definition of tracheomalacia. Most authors state that the cardinal finding is that of expiratory tracheal collapse. However, some expand the definition such that there must also be inspiratory tracheal dilatation. For the purpose of this article, the former broader definition is used.
Furthermore, some authors consider an overlap with the term excessive dynamic airway collapse (EDAC), however it is best thought that tracheomalacia describes a pathology whereby the cartilaginous structures of the trachea are weak, while EDAC is a mechanical description of resultant effect on the airway .
Epidemiology
The true incidence of tracheomalacia is uncertain, but has been identified in up to 23% of bronchoscopy and autopsy series, and 10% of CT series .
Clinical presentation
In many instances, the diagnosis is made incidentally on imaging of the chest. Patients frequently complain of shortness of breath, chronic cough and recurrent respiratory tract infection, although a causal link is difficult to establish in many cases .
Pathology
The underlying etiology is one of reduced or abnormal connective tissues in the trachea, particularly the cartilaginous rings.
Etiology
There are numerous causes of tracheomalacia, the commonest of which are:
- aging
- chronic obstructive pulmonary disease (COPD): sometimes considered as the most common acquired cause
- prolonged intubation, especially in those with tracheostomy
- chronic or recurrent infection
- asthma
Radiographic features
Plain radiograph
Plain inspiratory radiographs are usually normal or may demonstrate a dilated trachea. If expiratory films are obtained in lateral projection then the diagnosis may be evident, however, these are uncommonly performed.
CT
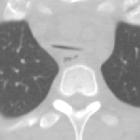
CT with inspiratory and expiratory phases is particularly useful in the assessment of tracheomalacia. Inspiratory only CT is unable to make the diagnosis; however, a dilated trachea (>3 cm), especially with posterior bowing of the membranous portion (thus becoming circular) may indicate over-compliance of the trachea and thus suggest the diagnosis.
During expiration, collapse of the trachea (dynamic tracheal collapse) is seen, with bowing of the posterior membranous portion anteriorly, creating a crescent shape in the axial plane . Typically a decrease of the anterior-posterior diameter by 50% or greater is used as a cut-off . Dynamic expiratory CT may show a significantly greater degree of airway collapse than a standard expiratory CT scan . During inspiration, the trachea may take the form of a crescent or moon (lunate trachea) which is highly sensitive but poorly specific for tracheomalacia .
Scanning during voluntary coughing has also been described and is probably more sensitive than using end-expiratory scanning, as the degree of increased intrathoracic pressure is greater .
It is also important to note that the degree of AP diameter reduction in a normal pediatric trachea is greater than that in adults, and thus care should be taken in correlating borderline findings with symptoms . In some instances, a cut-off of 70% reduction of AP diameter may be a more specific finding .
In most cases, the tracheal wall is normal or thin, although tracheomalacia with tracheal wall thickening has been reported in relapsing polychondritis .
Treatment and prognosis
In most cases, no treatment is required or offered. In severe cases, where significant symptoms can be ascribed to tracheomalacia, splinting of the membranous portion of the trachea with a variety of materials may be employed .
Differential diagnosis
As long as true dynamic expiratory collapse is seen, the diagnosis is usually obvious, however many underlying causes should be considered (see causes of tracheomalacia). In many instances, the diagnosis will be evident and thus features of each individual condition should be sought.
Siehe auch:
- Ösophagusatresie
- VACTERL-Assoziation
- saber-sheath trachea
- Williams-Campbell-Syndrom
- Differenzialdiagnosen bei Tracheomalazie
- kongenitale Tracheomalazie
- diffuse Trachealverengung
- angeborene ösophagotracheale Fistel
- Tracheobronchomalazie
- tracheobronchiale Chondritis
und weiter:


 Assoziationen und Differentialdiagnosen zu Tracheomalazie:
Assoziationen und Differentialdiagnosen zu Tracheomalazie:






