Ösophagusatresie


























Esophageal atresia refers to an absence in the continuity of the esophagus due to an inappropriate division of the primitive foregut into the trachea and esophagus. This is the most common congenital anomaly of the esophagus.
Epidemiology
It is thought to occur in ~1:3,000-4,500 live births .
Clinical presentation
Esophageal atresia may be suspected on antenatal ultrasound (see below) or in the neonate due to inability to swallow saliva or milk, aspiration during early feedings, or failure to pass a nasogastric tube into the stomach successfully.
Pathology
It results from a failure of the primitive foregut to divide into the trachea anteriorly and the esophagus posteriorly. This usually occurs at ~ the 4 week of gestation.
General pathogenesis includes teratogenic effects caused by early pregnancy use of antithyroid drugs
Genetics
Most cases have a sporadic occurrence .
Subtypes
It is frequently associated with a tracheo-esophageal fistula. As such, the types of esophageal atresia / tracheo-esophageal fistula can be divided into :
- proximal atresia with distal fistula: 85%
- isolated esophageal atresia: 8-9%
- isolated fistula (H-type): 4-6%
- double fistula with intervening atresia: 1-2%
- proximal fistula with distal atresia: 1%
See main article: esophageal atresia classification.
Associations
Esophageal atresias are frequently associated with various other anomalies (50-75% of cases). They include
- other intestinal atresias
- annular pancreas
- pyloric stenosis
- VACTERL association inclusive of congenital cardiac anomalies
- CHARGE syndrome
- increased incidence of chromosomal anomalies such as
Radiographic features
Plain radiograph
Chest x-ray:
- may show a dilated pharyngeal pouch
- the presence of air in the stomach and bowel in the setting of esophageal atresia implies that there is a distal fistula
- if an esophagogastric (feeding) tube insertion has been attempted this may show the tube blind looping and turning back at the upper thoracic part of the esophagus or heading into the trachea and/or bronchial tree
Fluoroscopy
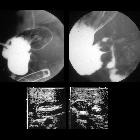
Contrast swallow may show contrast blindly ending and pooling in an esophageal stump and/or may show evidence of the tracheo-esophageal fistula. Fluoroscopy is particularly useful in demonstrating H-type fistula. A withdrawal esophagogram is performed for a H-type fistula. The patient is positioned prone and a horizontal beam is used, contrast material is injected through the nasogastric tube into the distal esophagus while the tube is slowly withdrawn under fluoroscopy . If the imaging study fails to locate the fistula while there is high suspicion then combined bronchoscopy and esophagoscopy is used . The gap between esophageal pouches is determined by inserting a Higer dilator through gastronomy into the distal esophagus and Repogle tube into proximal pouch; both tubes are radiopaque .
Antenatal ultrasound
- non-specific but may not show the expected shape and position of the stomach
- should be suspected if other VACTERL anomalies are seen
- polyhydramnios may be present particularly in cases where there is no concurrent fistulation
- the fetus may appear growth restricted
- the subtypes without a tracheo-esophageal fistula may be suspected in the context of persistent non-visualization of the fetal stomach
CT
- has been trialled for 3D detailed visualization of anatomy but not part of routine investigation
Treatment and prognosis
Surgical intervention with a re-anastomosis can be attempted post delivery. The prognosis is variable dependent on other associated anomalies.
Esophageal strictures secondary to surgical correction of esophageal atresia is a known complication of the procedure and usually requires further surgical correction.
Siehe auch:
- Down-Syndrom
- Pancreas anulare
- Herzfehler
- Analatresie
- VACTERL-Assoziation
- hypertrophe Pylorusstenose
- Polyhydramnion
- Trisomie 18
- ösophagotracheale Fistel
- Einteilung der Ösophagusatresie nach Vogt
- Duodenalatresie
- CHARGE-Syndrom
- chromosomale Anomalien
- Ösophagusatresie Typ II
- Trachealatresie
- Ösophagusatresie Typ 3b
- jejuno-ileal atresia
- growth restricted
- non visualisation of the fetal stomach
und weiter:
- Esophagus
- obstetric curriculum
- hemimetamere Segmentverschiebung
- Tracheomalazie
- Ileumatresie
- antenatal features of Down syndrome
- neonatal chest radiograph in the exam setting
- esophageal atresia with H-type tracheo-esophageal fistula
- Atresie
- Feingold syndrome
- H-type tracheo-oesophageal fistula with no atresia
- kongenitale Ösophagusstenose
- Klassifikation ösophagotrachealer Fisteln
- differential diagnosis of an absent fetal stomach on ultrasound
- angeborene ösophagotracheale Fistel
- esophageal atresia without tracheo-esophageal fistula
- Acute Respiratory Distress Syndrome neonatal


 Assoziationen und Differentialdiagnosen zu Ösophagusatresie:
Assoziationen und Differentialdiagnosen zu Ösophagusatresie: