fibrous cortical defect













































Fibrous cortical defects (FCD) are benign bony lesions and are a type of fibroxanthoma, histologically identical to the larger non-ossifying fibroma (NOF).
Epidemiology
Fibrous cortical defects typically occur in children (usually 2-15 years), and indeed are one of the most common benign bony lesions, which combined with non-ossifying fibromas are seen in up to 40% of skeletally immature children/adolescents . There is a male predilection by a ratio of 2:1 .
Clinical presentation
They are asymptomatic and self-limiting, completely healing by adulthood.
Pathology
Fibrous cortical defects macroscopically appear as fleshy, fibrous, yellow or tan-brown lesions with variable areas of hemorrhage .
Microscopic examination reveals the lesions to be highly cellular containing spindle-shaped cells on a background of stromal tissue in a prominent storiform pattern. Foamy histiocytes and multinucleated giant cells are also seen. Mitotic figures and/or cellular dysplasia should not be seen .
During the healing phase, there is an increase in osteoblastic activity as new bone replaces the defect, gradually being remodeled and completely disappearing .
Radiographic features
FCDs are benign lytic bone lesions, and, along with fibrous dysplasia share the F in the popular mnemonic FEGNOMASHIC.
They typically occur in the metaphysis or diametaphyseal junction and appear as small (<2-3 cm) lucent defects within the cortex that over time become sclerotic as they heal. They are typically located in the distal femur or proximal or distal tibia. They are much less frequently seen in the upper limb .
Importantly, there is no associated soft tissue mass .
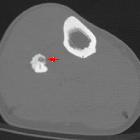
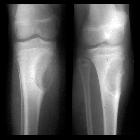
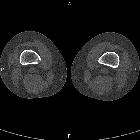
Plain radiograph and CT
- lucent intracortical defects
- outlined by a thin rim of sclerosis
- no involvement of the underlying medullary cavity
- no periosteal reaction
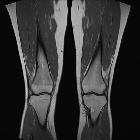
MRI
Signal characteristics include:
- T1: hypointense
- T2: variable, depending on the phase of healing
Nuclear medicine (bone scan)
Appearance depends on the phase of the lesion. In general they are negative; however, mild hyperemia and moderate bone uptake are present during healing. If extensive uptake or hyperemia is present, then an alternative diagnosis or superimposed fracture should be considered .
Treatment and prognosis
As these lesions are benign, characteristic in appearance and self-limiting, no treatment, biopsy or even follow-up is required in typical cases. If associated with pathological fracture (more common in non-ossifying fibromas) then cast immobilization until the fracture has healed, followed by biopsy with or without curettage, and bone grafting may be necessary .
History and etymology
Fibrous cortical defect was first described by Dallas Burton Phemister (1882-1951) , an American orthopedic surgeon in 1929 .
Differential diagnosis
Possible differential considerations include
- non-ossifying fibroma (NOF): larger (by definition >3 cm), bubbly
- cortical desmoid: posteromedial aspect of the distal femur
- osteoid osteoma: night pains
- osteomyelitis
- stress fracture
- intracortical osteosarcoma
Siehe auch:
- Osteoid-Osteom
- Fibröse Dysplasie
- nicht ossifizierendes Fibrom
- Aneurysmatische Knochenzyste
- Stressfraktur
- kortikales Desmoid
- Ossifizierendes Fibrom
- Chondromyxoidfibrom
- desmoplastisches Fibrom
- Fokale kortikale Dysplasie
- lytic bone lesion (mnemonic)
- ausgeheiltes nicht ossifizierendes Fibrom (NOF)
- Fibroxanthom des Knochens
- fokale fibrokartilaginäre Dysplasie
- Fibroxanthom
und weiter:


 Assoziationen und Differentialdiagnosen zu fibröser Kortikalisdefekt:
Assoziationen und Differentialdiagnosen zu fibröser Kortikalisdefekt: