gynecomastia































Gynecomastia refers to a benign excess of the male breast tissue, that is usually reversible. It is not a risk factor per se for developing male breast cancer.
Epidemiology
While it can occur at any age, it tends to have greater prevalence in two groups: adolescent boys and older men (some publications describe a trimodal age distribution, occurring in neonatal, pubertal, and elderly males ). Prevalence of "asymptomatic" gynecomastia ranges around :
- neonates: 60-90%
- adolescents: 50-60%
- men aged 50 to 69 years: up to 70%
Prevalence of "symptomatic" cases is markedly lower.
Clinical presentation
Palpation usually demonstrates a palpable, tender, firm, mobile, disc-like mound of tissue .
Pathology
In gynecomastia, there is enlargement of the male breast due to benign ductal and stromal proliferation. A hallmark of gynecomastia is its central symmetric location under the nipple. Gynecomastia in most cases tends to be unilateral and/or asymmetrical .
The imbalance between estrogen action relative to androgen action at the breast tissue level appears to be a key etiological factor in gynecomastia.
Etiology
The causes of gynecomastia are many and include:
- hormonal
- neonatal: maternal estrogens
- pubertal: high estradiol levels
- elderly: decline in testosterone levels
- hypogonadism/androgen deficiency states:
- Klinefelter syndrome
- anorchism
- testicular failure, e.g. testicular cancer
- drugs
- diethylstilbestrol
- spironolactone
- thiazide diuretics
- digoxin
- anabolic steroids
- estrogen treatment
- flutamide
- finasteride
- isoniazid
- ergotamine
- narcotics:
- marijuana
- heroin
- cimetidine
- nifedipine
- reserpine
- efavirenz
- methyldopa
- theophylline
- systemic disorders
- advanced alcoholic cirrhosis
- chronic pulmonary disease, e.g. emphysema, tuberculosis
- haemodialysis in chronic renal failure
- hyperthyroidism
- malnutrition
- tumors: particularly oestrogenic tumors
- adrenal carcinoma
- hepatoma
- lung cancer
- pituitary adenoma
- testicular cancer: including sex-cord stromal, and germ cell tumors
- idiopathic
Histology
There can be three histological forms:
- florid
- intermediate
- fibrotic
Radiographic features
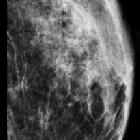
Mammography
May appear as an increased sub-areolar density, which may be flame-shaped.
Three mammographic patterns of gynecomastia have been described representing various degrees and stages of ductal and stromal proliferation. They are:
- nodular pattern
- dendritic pattern
- diffuse glandular pattern
Early nodular gynecomastia (florid phase) is seen in patients with gynecomastia for less than 1 year. At mammography, there is often a nodular subareolar density.
Chronic dendritic gynecomastia (quiescent phase) is seen in patients with gynecomastia for longer than 1 year. Fibrosis becomes the dominant process and is irreversible. Mammograms this phase typically show a dendritic subareolar density with posterior linear projections radiating into the surrounding tissue toward the upper-outer quadrant.
Diffuse glandular gynecomastia is commonly seen in patients receiving exogenous estrogen. At mammography, there is enlargement of the breast and diffuse density with both dendritic and nodular features.
Ultrasound
Focal gynecomastia can variably appear as a retroareolar, triangular, hypoechoic (~80%) mass.
In early nodular gynecomastia, there can be subareolar fan or disc-shaped hypoechoic nodule surrounded by normal fatty tissue.
In diffuse glandular gynecomastia, both nodular and dendritic features are seen surrounded by diffuse hyperechoic fibrous breast tissue.
In chronic dendritic gynecomastia, there is often a subareolar hypoechoic lesion with an anechoic star-shaped posterior border, which can be described as fingerlike projections or "spider legs" insinuating into the surrounding echogenic fibrous breast tissue.
Differential diagnosis
- pseudogynecomastia: involves breast enlargement (usually bilateral) caused by an excess of adipose tissue, which is not necessarily associated with constitutional obesity
- male breast cancer :
- unilateral fixed painless irregular hard mass
- may occur remotely from the areola (gynecomastia does not)
- skin thickening and tethering
See also
Siehe auch:
- Tuberkulose
- Leberzirrhose
- hepatozelluläres Karzinom
- Hypophysenadenom
- Nebennierenrindenkarzinom
- Mammakarzinom beim Mann
- Klinefelter-Syndrom
- male breast disease
- Emphysem
- maligne Neoplasien des Hodens
- pseudogynaecomastia
und weiter:


 Assoziationen und Differentialdiagnosen zu Gynäkomastie:
Assoziationen und Differentialdiagnosen zu Gynäkomastie:






