pleural metastases








Pleural metastases account for the vast majority of malignant lesions of the pleura and are more common than malignant mesothelioma.
Clinical presentation
The infiltration of the pleura usually manifests as pleural effusion, which is the first manifestation of pleural metastasis. In addition to the symptoms and systemic manifestations of neoplastic disease, as in general conditions, anorexia or weight loss, one of the most constant symptoms is dyspnea, which occurs >50% of patients with malignant pleural effusion.
Pathology
Pleural metastases usually affect the visceral and parietal pleura, pleural effusion almost always occurs due to impaired lymphatic drainage or capillary permeability increased by inflammation or rupture of the endothelium.
Etiology
The adenocarcinoma histological type is the most likely to produce metastasis in the pleura. The most common primaries to result in pleural metastases include:
- lung cancer: may account for up to 40% of pleural metastases
- breast carcinoma
- may account for ~20% of pleural metastases
- commonly gives a pleural effusion
- ovarian cancer
- lymphoma: may account ~10% of metastases
- gastric carcinoma
- invasive thymoma
- neuroblastoma
- cutaneous malignant melanoma
- renal cell carcinoma
- bladder cancer
- osteosarcoma
- endometrial carcinoma
Radiographic features
Although pleural effusion is often the major component of metastatic disease to the pleura, other findings include pleural nodules or extensive pleural thickening similar to that of mesothelioma.
Plain radiograph
Features on chest x-ray include
- pleurally-based masses
- pleural thickening
- pleural effusion
- +/- rib destruction
- +/- hilar/mediastinal lympadenopathy
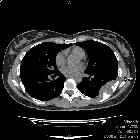
CT
CT is the method of choice and may show nodules not seen on chest X-ray due to pleural effusion. The pleural metastases usually manifest as enhancing nodular or lenticular masses. Other findings seen on CT are enlarged mediastinal lymph nodes, lung nodules, rib lesions, or subcutaneous extention.
Differential diagnosis
It can be difficult to differentiate pleural metastasis from primary pleural malignancy such as malignant mesothelioma since both can cause pleural effusions, pleural nodules, and isolated, diffuse or nodular thickening.
See also
- tumors of the pleura
- pleural carcinomatosis
- pleural seeding of tumors
Siehe auch:
- pleurale Lipome
- Pleurakarzinose
- solitärer fibröser Tumor der Pleura
- Pleuramesotheliom
- maligne pleurale Tumoren
- einzelne Pleuraraumforderung
- Tumoren der Pleura
und weiter:


 Assoziationen und Differentialdiagnosen zu pleurale Metastasen:
Assoziationen und Differentialdiagnosen zu pleurale Metastasen:





