embryonal tumor with multilayered rosettes










Embryonal tumors with multilayered rosettes (ETMR) are rare small round blue cell tumor of the central nervous system and are one of the most aggressive brain tumors usually encountered in children.
Terminology
Previously embryonal tumors with multilayered rosettes (ETMR) were known as embryonal tumor with abundant neuropil and true rosettes (ETANTR). This term has, however, been removed from the 2016 update to WHO classification of CNS tumors in favor of embryonal tumors with multilayered rosettes (ETMR) which incorporates not only ETANTR but also ependymoblastoma and CNS PNET which have also been removed from the classification) . This has resulted due to the presence of amplification of the C19MC region on chromosome 19 in both CNS PNET and ETANTR, suggesting that these are the one entity with variable growth pattern .
Epidemiology
ETMR occurs in children aged 4 and under, mostly in children under 2, and is more common in girls, unlike the other CNS embryonal tumors, in which boys are equally or more commonly affected.
Clinical presentation
The clinical features are determined by the location and extent of the tumor. Most are supratentorial in location, a few are infratentorial, and they are very rarely encountered in the spinal cord.
Increased intracranial pressure, seizures, hemiparesis, cerebellar signs, cranial nerve palsies, and other neurologic deficits have all been reported.
Pathology
Embryonal tumors with multilayered rosettes (ETMR) are characterized by undifferentiated neuroepithelial cells resembling those of classic CNS PNET, abundant well-differentiated neuropil, and ependymoblastic rosettes scattered throughout paucicellular regions of neoplastic neuropil. Unlike medulloblastoma, ETMR has no epithelial-like formation. Instead, it has a very characteristic ependymoblastic rosettes in both highly cellular as well as acellular areas.
Recently amplification of the C19MC region on chromosome 19 (19q13.42) has been identified as characteristic of these tumors, along with what historically had been termed CNS PNET. As a result, both ETANTR and CNS PNET have been removed from the 2016 update of the WHO classification of CNS tumors and been replaced by the term embryonal tumor with multilayered rosettes (ETMR), C19MC-altered (or ETMR-NOS if C19MC amplification is absent) .
Radiographic features
MRI
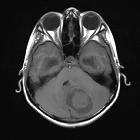
The tumor appears as a large, demarcated, solid mass featuring patchy or no contrast enhancement, with surrounding edema, often with significant mass effect. A minority of the reported cases have shown cystic components and microcalcifications.
- T1: decreased intensity
- T2: increased intensity
- T1 C+ (Gd): patchy or no contrast enhancement
MR spectroscopy shows choline peak and a high ratio of choline/aspartate suggesting hypercellularity of the tumor.
Treatment and prognosis
Current treatment options for ETMR include surgical resection, systemic chemotherapy and craniospinal radiation (when appropriate).
Unfortunately, the prognosis is dismal, with most recent articles reporting ~75% of cases have died within the median survival of 9 months.
Differential diagnosis
The differential diagnosis varies according to the location of the tumor. The general imaging differential for the brain stem and infratentorial ETMR include:
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Embryonaler Tumor mit mehrreihigen Rosetten:
Assoziationen und Differentialdiagnosen zu Embryonaler Tumor mit mehrreihigen Rosetten: