Struma ovarii Tumor



Struma ovarii tumor is a subtype of an ovarian teratoma and is composed entirely or predominantly of thyroid tissue and containing variable-sized follicles with colloid material.
Epidemiology
It accounts for 0.3-1% of all ovarian tumors and ~3% of all mature cystic teratomas .
Clinical presentation
Approximately 5-8% of cases can show symptoms or signs of thyrotoxicosis.
Pathology
To qualify as a struma ovarii tumors more than 50% of the tumor should be composed of thyroid tissue .
The gross pathologic appearance of struma ovarii differs from that of mature cystic teratomas where struma ovarii consist of amber-colored thyroid tissue, with hemorrhage, necrosis, and fibrosis.
Radiographic features
While imaging features can be non-specific and overlap with other ovarian neoplasms, ultrasound and CT usually demonstrate a complex adnexal lesion with multiple cystic and solid areas, reflecting the gross pathologic appearance of the tumor . Ascites may be present in up to a third of cases .
CT
On CT scans they are most often seen as smooth marginated multicystic masses with a high attenuation on precontrast scans and no or moderate cyst wall enhancement .
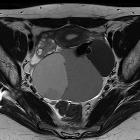
Pelvic MRI
May be seen as a multiloculated cystic mass, with solid parts. The cystic spaces can demonstrate both high and low (from gelatinous colloid ) signal intensity on T1 and T2 weighted images.
The presence of areas of very low signal intensity on T2-weighted images, due to the viscous colloid material is sometimes considered as suggestive for the presence of struma ovarii tumor.
- T1 C+ (Gd): the solid portions may show enhancement
Treatment and prognosis
Treatment is with surgical resection. The vast majority of struma ovarii tumors (90-95% ) tend to be benign and therefore carry a good prognosis.
History and etymology
First described by R Boettin in 1889 .
See also
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Struma ovarii Tumor:
Assoziationen und Differentialdiagnosen zu Struma ovarii Tumor:

