Chorea-Akanthozytose
Chorea-acanthocytosis (ChAc) is an autosomal recessive, progressive neurological disorder. It is the commonest of the four core neuroacanthocytosis syndromes (NAS). Symptomatology includes movement disorder, acanthocytosis, elevated creatinine kinase, and atrophy of the basal ganglia.
Epidemiology
Estimates suggest one thousand cases of ChAc, worldwide .
Clinical presentation
Symptom onset occurs in early adulthood at a median of 30 years of age, but ranging from 20th to the 70th decade . Approximately one-third of patients initially experience generalized or complex partial seizures, which may precede neurological dysfunction by a decade . In addition, psychiatric conditions, often depression or obsessive-compulsive symptoms, and parkinsonism may also be presenting features of ChAc . The peculiar finding of "feeding dystonia" is pathognomonic of ChAc: upon food touching the tongue, the tongue protrudes and forces the bolus out. Chorea typically affects the arms, legs and shoulder and pelvic girdles . Movement disorder with choreiform and dystonic components affects gait. Specifically, the presence of "rubber-man appearance", truncal instability and loss of axial tone with sudden, violent flexion and extension spasms, is highly suggestive of ChAc .
Pathology
Etiology
Mutations in the vacuolar protein sorting 13 homolog A (VPS13A) gene, located on chromosome 9q21, have been demonstrated in lineages affected by ChAc . A variety of mutations occur, with genomic analysis of 11 ChAc families identifying 16 disease-causing mutations in VPS13A .
The mechanism underlying pathogenesis is unclear but thought to involve protein sorting . Indeed, the biological process linking acanthocytosis, basal ganglia degeneration, raised creatinine kinase and monogenetic mutations in protein sorting genes is yet to be elucidated in any of the NAS.
Radiographic features
MRI
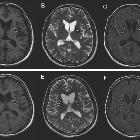
Bilateral, near symmetrical, atrophy of the head of the caudate nucleus is common across affected families, and can be seen on standard T1 or T2-weighted MRI . To a lesser extent, atrophic changes occur in the putamen, globus pallidus and substantia nigra .
Treatment and prognosis
Treatment is symptomatic, with quality of life most profoundly improved by the management of psychiatric symptoms . Progression of disease is variable. Typically, slow progression occurs over 15-30 years .
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Chorea-Akanthozytose:
Assoziationen und Differentialdiagnosen zu Chorea-Akanthozytose: