CT pulmonary angiogram (technique)

Pulmonary
embolism in computertomography. The patient suffered from portal vein thrombosis a year later.

Pulmonary
embolism • Pulmonary embolism - Ganzer Fall bei Radiopaedia

CT pulmonary
angiogram (protocol) • Pulmonary embolism on suboptimal CTPA (spectral low monoE) - Ganzer Fall bei Radiopaedia

CT pulmonary
angiogram (protocol) • Pulmonary embolism (spectral CTPA) - Ganzer Fall bei Radiopaedia

CT pulmonary
angiogram (protocol) • Normal spectral CTPA - Ganzer Fall bei Radiopaedia

CT pulmonary
angiogram (protocol) • Saddle pulmonary embolus - Ganzer Fall bei Radiopaedia

CT pulmonary
angiogram (protocol) • Normal CTPA - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Pulmonary embolism - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Pulmonary embolism - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Pulmonary embolism - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Pulmonary embolus - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Extensive acute pulmonary emboli with right heart strain - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Incidental pulmonary embolism - Ganzer Fall bei Radiopaedia


Pulmonary
embolism • Pulmonary embolism - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Saddle pulmonary embolism - Ganzer Fall bei Radiopaedia

Pulmonary
embolism • Acute pulmonary embolism - Ganzer Fall bei Radiopaedia
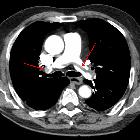
A large
pulmonary embolism at the bifurcation of the pulmonary artery (saddle embolism).


Thorax CT of
a 74-year-old man with a long-standing pulmonary embolism (having lasted 3 months) of the artery of the right lower lobe, secondary to a leg fracture, and with long-standing hemoptysis. It shows the embolism, as well as a pulmonary infarction seen as a reverse halo sign. Further information: Reverse halo sign

This image
is part of a series which can be scrolled interactively with the mousewheel or mouse dragging. This is done by using Template:Imagestack. The series is found in the category Pulmonary embolism - CT - case 001. Reitender Thrombus bei Lungenembolie. Genaugenommen sind es hier mehrere zentrale von links nach rechts reitende Thromben. Die linken Hauptstämme sind weitestgehend okkludiert.

CT pulmonary
angiogram (protocol) • Aortic dissection (CTPA) - Ganzer Fall bei Radiopaedia
The computed tomography pulmonary angiogram (CTPA/CTPE) is a commonly performed diagnostic examination to exclude pulmonary emboli. Each radiology department will have a slightly different method for achieving the same outcome, i.e. adequate enhancement of the pulmonary trunk and its branches.
There are two principal approaches for performing a CTPA of high diagnostic quality:
- a small ‘test’ quantity of contrast is injected and sequential axial slices at a set region of interest are acquired to calculate the time of peak contrast enhancement and determine an optimal scan delay
- sequential axial slices at a set region of interest are conducted during the contrast injection until a threshold enhancement is met, triggering a diagnostic scan
NB: This article is intended to outline some general principles of protocol design. The specifics will vary depending on CT hardware and software, radiologists' and referrers' preference, institutional protocols, patient factors (e.g. allergy) and time constraints.
Indications
Contraindications
- previous severe reactions to iodinated contrast
- non-compliance
Technique
Bolus tracking
- patient position
- supine with their arms above their head
- scout
- apices to diaphragm
- scan extent
- apices to diaphragm
- scan direction
- caudocranial
- contrast injection considerations
- monitoring slice (region of interest)
- below the carina at the level of the pulmonary trunk with an ROI on the pulmonary artery
- threshold
- 100 HU
- volume
- 60 mL of non-ionic contrast with a 100 mL saline chaser at 4.5/5 mL/s
- monitoring slice (region of interest)
- scan delay
- minimal scan delay
- respiration phase
- inspiration
Test bolus
- patient position
- supine with their arms above their head
- scout
- apices to diaphragm
- scan extent
- apices to diaphragm
- scan direction
- caudocranial
- contrast injection considerations
- test bolus
- contrast volume
- 20 mL of non-ionic contrast with a 10 mL saline chaser at 4.5/5 mL/s
- monitoring slice (region of interest)
- below the carina at the level of the pulmonary trunk with an ROI on the pulmonary artery
- monitor contrast enhancement peak over time via a time-enhancement curve
- contrast volume
- calculating scan delay
- as the time-enhancement curve will only begin recording after the scan delay. A widely accepted formula for calculating the scan delay is :
- peak contrast enhancement (time-enhancement curve) + scanner's diagnostic scan delay
- as the time-enhancement curve will only begin recording after the scan delay. A widely accepted formula for calculating the scan delay is :
- contrast volume (diagnostic scan)
- 60 mL of non-ionic contrast with a 100 mL saline chaser at 4.5/5 mL/s
- scan delay
- peak contrast enhancement (time-enhancement curve) + scanner's diagnostic scan delay
- respiration phase
- inspiration
Practical points
- what constitutes as a diagnostic CTPA based on enhancement varies from site-to-site
- changing the scan direction to caudocranial has been shown to better demonstrate the lower lobes whilst alleviating artefact from the contrast bolus in the SVC
- use of monoenergetic reconstruction of CTPA studies with suboptimal enhancement has been shown to increase enhancement of the pulmonary trunk
- use of high-pitch-scanning in non-obese patients can see a reduction in contrast use to as low as 12 mL
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Lungenembolie-CT:
Assoziationen und Differentialdiagnosen zu Lungenembolie-CT:
