Endometriose der Harnblase

Endometriose der Harnblase
Endometriose Radiopaedia • CC-by-nc-sa 3.0 • de
Endometriomas, also known as chocolate cysts or endometriotic cysts, are a localized form of endometriosis and are usually within the ovary. They are readily diagnosed on ultrasound, with most demonstrating classical radiographic features.
Epidemiology
These occur in women of reproductive age.
Pathology
Endometriomas contains dark degenerated blood products following repeated cyclical hemorrhage. The cysts may be up to 20 cm in size although they are usually smaller (2-5 cm).
Location
Typical locations include:
- ovaries: ~75%
- anterior/posterior cul-de-sac: ~70%
- posterior broad ligament: ~50%
- uterosacral ligaments: ~35%
- uterus: ~10 %
- colon: ~5%
Radiographic features
Plain radiograph
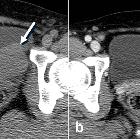
Not usually helpful in diagnosis; ~10% of endometriomas can calcify.
Ultrasound
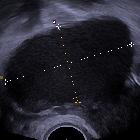
The appearances of endometriomas can be quite variable. The classical example is a unilocular cyst with acoustic enhancement with diffuse homogeneous ground-glass echoes as a result of the hemorrhagic debris. This appearance occurs in 50% of cases .
Less typical features include :
- multiple locules (~85% will have <5 locules)
- hyperechoic wall foci (present in 35%)
- cystic-solid lesion (~15%) or purely solid lesion (1%)
- anechoic cysts (rare; 2%)
MRI
Signal characteristics vary according to the age of any complicating hemorrhage :
- T1
- typically, lesions appear hyperintense while acute hemorrhage occasionally appears hypointense
- endometriomas with high T1 signal characteristically do not show loss of signal on T1 fat suppressed sequence, which is important for differentiating it from mature cystic teratoma of the ovary
- T2
- typically hypointense owing to the presence of deoxyhemoglobin and methemoglobin (shading sign), which is very suggestive of endometrioma
- T2 dark spot sign is specific for chronic hemorrhage and is helpful in diagnosing endometriomas
- old hemorrhage occasionally appears hyperintense
- DWI
- variable restricted diffusion
- T1C+
- may have wall enhancement
- the presence of an enhancing mural nodule is suggestive of malignant transformation
Treatment and prognosis
Although endometriomas are usually a benign entity, there is an ~1% rate of malignant transformation. Endometrioid tumors of the ovary and clear cell adenocarcinoma are the most common histological pattern seen . They are mostly seen in women >40 years after several years of latency, with endometriomas larger than 9 cm . Malignant transformation is uncommon in masses <6 cm.
If not surgically excised, follow-up should be at least yearly . GnRH agonists may be used for medical management.
Differential diagnosis
General imaging differential considerations include:
- hemorrhagic ovarian cyst
- brighter on T2-weighted images
- an absence of the "shading sign"
- ovarian dermoid cyst
- will show fat suppression on fat suppressed sequences on MRI
- cystic neoplasm
- tubo-ovarian abscess
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Endometriose der Harnblase:
Assoziationen und Differentialdiagnosen zu Endometriose der Harnblase: