fibrillary astrocytoma
Fibrillary astrocytomas are the most common type of diffuse low grade astrocytoma and as of the 2016 update to WHO classification of CNS tumors it no longer exists as a distinct entity, having been incorporated into the generic term diffuse astrocytoma .
Terminology
Unlike the other variants of diffuse low grade gliomas (e.g. gemistocytic astrocytoma, protoplasmic astrocytoma, oligoastrocytoma) or the focal low grade gliomas (e.g. pilocytic astrocytoma, subependymal giant cell astrocytoma) they are often merely referred to as a low grade glioma.
Epidemiology
Typically patients diagnosed with low grade infiltrative astrocytomas are young adults (mean 35 years of age) . A male predilection is described (M:F ~1.5:1) .
Clinical presentation
The most common presenting feature (~40% of cases) is seizures. This is particularly the case in adults. Headaches are often also present. Depending on the size of the lesion and its location other features may be present, e.g. hydrocephalus, focal neurological dysfunction including personality change.
Pathology
The fibrillary astrocytomas are predominantly composed of a tumor matrix rich with neuroglial fibrils, which give the tumor its name and firm consistency . Within the tumor matrix are embedded neoplastic fibrillary astrocytes with mild nuclear atypia (enlarged, irregular contour, hyperchromasia and coarsened nuclear chromatin pattern) and a low cellular density . The nuclei are elongated and appear "naked" .
Often microcystic spaces containing mucinous fluid are present . Mitoses, microvascular proliferation and necrosis are absent (if present they suggest a high grade tumor). Like all tumors derived from astrocytes, fibrillary astrocytomas stain with glial fibrillary acidic protein (gFAP) .
Radiographic features
MRI is the modality of choice for characterizing these lesions, and in the case of smaller tumors, they may be subtle and difficult to see on CT, especially as they tend not to enhance.
CT
Typically fibrillary low grade infiltrating astrocytomas appear as isodense or hypodense regions of positive mass effect, usually without any enhancement (in fact presence of enhancement would suggest high grade, e.g. WHO III or IV tumors.
Calcification is infrequently seen (10-20% of cases) but is more common in mixed tumors relating to an oligodendroglial components (i.e. oligoastrocytoma).
Cystic or fluid attenuation components are also encountered although this is far more common in gemistocytic and protoplasmic variants.
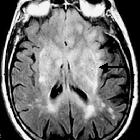
MRI
- T1: isointense to hypointense compared to white matter
- T2: hyperintense
- T1 C+ (Gd): usually little or no enhancement
- MR spectroscopy: elevated choline:creatine ratio
- MR perfusion: no elevation of rCBV
Treatment and prognosis
Treatment depends on clinical presentation, size of the tumor and location. In general the options are:
- observe
- biopsy to confirm diagnosis and observe
- resection
- radiotherapy
- chemotherapy may have a role in recurrent/de-differentiated tumors
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu fibrillary astrocytoma:
Assoziationen und Differentialdiagnosen zu fibrillary astrocytoma: