gastric varices

Gastric varices are an important portosystemic collateral pathway, occurring in ~20% of patients with portal hypertension. They are considered distinct from esophageal varices in that they have a propensity to hemorrhage at comparatively lower portal pressures , and are also associated with higher mortality rate with hemorrhage (range 14-45%) .
Clinical presentation
Patients may present with symptoms and signs of upper gastrointestinal bleeding or hypovolemia such as:
- coffee-ground vomit
- melena
- syncope
- shock
Patients will generally have a history of cirrhosis and may have other symptoms of chronic liver disease.
Pathology
Gastric varices occur due to elevated portal venous pressure, and represent a collateral flow pathway from the congested portal system to systemic veins. They commonly co-occur and may be continuous with esophageal varices .
The gastric varix itself usually represents a dilated left gastric or posterior gastric vein.
Afferent inflow is most commonly from :
- left gastric vein
- posterior gastric vein
- gastroepiploic vein (rare) - mostly occurring after prior intervention
Efferent outflow is most common through :
- gastrorenal shunt (to left renal vein)
- often communicates with small retroperitoneal veins
- may or may not communicate with the phrenicopericardial or intercostal veins
- rarely communicates with the ascending lumbar, vertebral plexus, or azygos veins
- gastro-caval shunt (to suprarenal IVC)
- often communicates with the phrenicopericardial and intercostal veins
- rarely communicates with the azygos vein
- fundus-inferior phrenic vein
Classification
The most common (Sarin) classification scheme characterizes gastric varices by their co-occurrence with esophageal varices and anatomic location :
- gastric and esophageal varices (GOV)
- type 1 (GOV1) - at lesser curvature
- type 2 (GOV2) - at gastric fundus
- isolated gastric varices (IGV)
- type 1 (IGV1) - at gastric fundus
- type 2 (IGV2) - other gastric or early duodenal location
In 2003, Kiyosue proposed a classification system intended to guide intervention by BRTO-type techniques. With this in mind, gastric varices may be characterized by inflow and outflow patterns:
Inflow pattern (following outflow occlusion)
- Type 1 - stagnant varices flow
- Type 2 - shifting flow between separate gastric varices
- Type 3 - continued efferent flow via separate draining vein, despite occlusion
Outflow
- Type A - drained by a single large shunt
- Type B - drained by a single shunt + smaller collateral veins
- Type C - drained by both gastro-renal and gastro-caval shunts
- Type D - not continuous with a shunt (multiple smaller collaterals)
Radiographic features
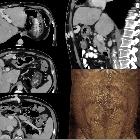
CT
CT with intravenous contrast enhancement is helpful in confirming the presence of gastric varices and identifying their cause. Findings include well-defined clusters of rounded and tubular enhancing vessels. Other findings consistent with portal hypertension may be found .
Treatment and prognosis
Management of gastric varices is also distinct from esophageal varices due to the anatomy. Endoscopic clipping or sclerosing are typically first line treatments, although interventional radiology techniques such as TIPS and BRTO are important therapeutic adjuncts. Indeed, BRTO is first-line therapy for gastric variceal hemorrhage in some Asian countries .
Siehe auch:
- portosystemische Umgehungskreisläufe
- portale Hypertension
- Ösophagusvarizen
- transjugulärer intrahepatischer portosystemischer Shunt
und weiter:


 Assoziationen und Differentialdiagnosen zu Fundusvarizen:
Assoziationen und Differentialdiagnosen zu Fundusvarizen: