High-velocity penetrating brain injury










High-velocity penetrating brain injuries, in practical terms most often due to cranial gunshot injuries, are a form of penetrating traumatic brain injuries, which are much less common than blunt traumatic brain injuries and distinguished from low-velocity penetrating brain injuries (such as stabbings) by the amount of kinetic energy deposited in the skull and brain parenchyma, which in turn has implications for the pattern and severity of injury.
Because the vast majority of high-velocity penetrating brain injuries are due to gunshot wounds, the terms are used interchangeably in this article.
Epidemiology
The incidence of gunshot injuries to the head is increasing in some countries, due to the ease of accessibility of firearms. In the civilian population, suicide and criminal activity account for the majority of cases and young male adults remain the most at risk .
Pathology
Damage to the bone and soft tissues of the head by high-velocity projectiles is dependent on a number of factors, such as shape and size, however, the dominant factor is the amount of kinetic energy they deposit as they traverse tissues. Total energy is proportional to the mass of the object times the square of its velocity (E = 1/2mv). In other words, most of the kinetic energy available is due to velocity, explaining why a small bullet can do far more damage than a much larger object (e.g. knife blade) and why the patterns of injury for high-velocity objects is different to low-velocity ones. Both with cause direct damage as they traverse brain, however, high-velocity projectiles will also be able to impart significant kinetic energy to bone fragments and cause a cavitary shockwave in their wake which can damage tissue at considerable distances from the injury tract .
The pathways taken by high-velocity projectiles (e.g. bullets) can be divided into five patterns with distinctive patterns of injury :
Radiographic features
As is the case with low-velocity penetrating brain injuries, CT and CT angiography are the cornerstones of emergent imaging of all patients with penetrating injuries. Plain films have largely been replaced by CT and MRI is usually not indicated until later in the admission if at all. Of particular importance is the possibility that the penetrating material is ferromagnetic precluding safe MRI.
Many of the imaging features for high-velocity injuries are similar as those for low-velocity penetrating brain injuries and thus are solely discussed here to avoid repetition.
Note: Please see the main article "imaging of gunshot injuries" for a general description of imaging features.
CT
A number of features need to be assessed in patients with penetrating injuries, with care taken to carefully document findings as often these scans will be used in medicolegal proceedings.
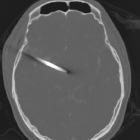
Skull
The entry and exit wounds can be identified paying attention to the bone “beveling”. An inward beveling of the inner skull table is supportive of the entry wound, whereas the outward beveling of outer skull table suggests the exit wound. Often there is not an exit wound, especially in incomplete metal jacket bullets (e.g. hollow-point tip) that are designed to fragment and lose kinetic energy along their path .
Location and extension of linear fractures as well as any non-penetrating fractures from coexisting blunt head trauma.
Foreign bodies
Location, number (sometimes difficult if highly fragmented) and density (usually metal in high-velocity injuries) of fragments, particularly in relation to eloquent parts of the brain or vessels.
Parenchyma and hematomas
The direction of tract(s) and the key structures they traverse along with the amount of hemorrhage, particularly if there are sizable hematomas that need evacuation. This is particularly the case for extra-axial hemorrhages that may occur due to vascular injury.
CT angiography
Angiographic imaging is used when there is evidence or suspicion of intracranial vascular injury. Projectiles or penetrating injuries that have traversed the base of skull or orbits have a high incidence of vascular injury .
CTA may demonstrate a CTA spot sign indicating active hemorrhage at the time of the scan, as seen in non-traumatic intraparenchymal hemorrhage, which correlates with a worse prognosis.
Vascular injuries include transsection, pseudoaneurysm, dissection or thromboembolic occlusion.
Digital subtraction angiography
DSA is used when CTA fails to demonstrate a vascular injury and the suspicion remains high or endovascular treatment is being considered. Delayed DSA may also be performed to assess for complications such as AV fistula .
Treatment and prognosis
Unsurprisingly, mortality is high. In civilian shootings, approximately 20% survive the initial injury, and of those, ~50% (range 30-68%) survive .
Complications
There are numerous complications ranging from instant to delayed :
- infection: cerebral abscess, meningitis, etc.
- CSF leak
- arterial injury: dissection, transsection, false aneurysm, etc.
- venous injury: dural venous sinus thrombosis
- infarct
- hydrocephalus
- bullet migration

