Hydrozele
















Hydroceles are acquired or congenital serous fluid collections between the layers of the tunica vaginalis surrounding a testis or spermatic cord. They are the most common form of "testicular" enlargement and present with painless enlargement of the scrotum. On all modalities, hydroceles appear as simple fluid, unless complicated by infection or hemorrhage.
Epidemiology
Hydroceles can be diagnosed at any age, with congenital hydrocele being more common in children.
Clinical presentation
Most hydroceles are acquired and present with progressing painless scrotal mass. During the physical examination, hydrocele characteristically transilluminates when evaluated with a light source. They can become painful if infected (see pyocele).
Pathology
Etiology
Congenital
There are two main subtypes of congenital hydrocele:
- communicating hydrocele
- spermatic cord hydrocele
In the communicating type, fluid collects around a patent processus vaginalis which failed to successfully obliterate.
The spermatic cord hydrocele is further subdivided into:
- encysted type (spermatic cord cyst): no communication with the peritoneum or tunica vaginalis
- funicular type (funiculocele): communicates with the peritoneum at the internal ring and doesn't surround the testis
- more common in children and premature infants
Acquired
Radiographic features
Ultrasound
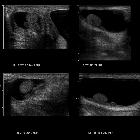
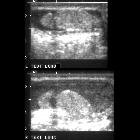
Ultrasound is the first modality usually used to evaluate hydrocele, which presents as a simple fluid collection. It is avascular on Doppler evaluation. It may contain septations, calcifications or cholesterol .
Communicating, infantile and vaginal hydroceles will be seen intimately surrounding the adjacent testicle. In contrast, spermatic cord hydroceles such as funicular hydrocele (funiculocele) and encysted hydrocele will not surround the testis, rather being found along the spermatic cord.
Hydroceles can also appear larger with straining (Valsalva maneuver) . They may contain fibrous adhesions, giving a beaded appearance to the spermatic cord (pachyvaginalitis)
MRI
On MRI, signal characteristics of the hydroceles are
- T1: low signal
- T2: high signal
This represents the serous fluid of an uncomplicated hydrocele.
Treatment and prognosis
In infants, most hydroceles (around 90%) resolve spontaneously, and they are thought to result from incomplete obliteration of the processus vaginalis. It is important to assess for any associated herniations in these patients.
Differential diagnosis
Imaging differential considerations include
Rarely, a scrotal tunica cyst or scrotal mesothelioma can look like a hydrocele, but they are usually easily distinguishable.
See also
Siehe auch:
- Hydrozele im Nuck'schen Kanal
- Spermatozele
- Inguinalhernie
- skrotale Hämatozele
- Hydrozele des Samenstrangs
und weiter:


 Assoziationen und Differentialdiagnosen zu Hydrozele:
Assoziationen und Differentialdiagnosen zu Hydrozele:



