Jefferson-Fraktur















Jefferson fracture is the eponymous name given to a burst fracture of the atlas. It was originally described as a four-part fracture with double fractures through the anterior and posterior arches, but three-part and two-part fractures have also been described.
Pathology
Mechanism
A typical mechanism of injury is diving headfirst into shallow water. Axial loading along the axis of the cervical spine results in the occipital condyles being driven into the lateral masses of C1. The Jefferson fracture is not normally associated with neurological deficit although spinal cord injury may occur if there is a retropulsed fragment affecting the cervical cord.
Associations
- 50% are associated with other C-spine injuries
- 33% are associated with a C2 fracture
- 25-50% of young children have a concurrent head injury
- vertebral artery injury (blunt cerebrovascular injury, BCVI)
- extra-cranial cranial nerve injury
Radiographic features
Plain radiograph
Radiographs will show asymmetry in the odontoid view with the displacement of the lateral mass(es) away from the odontoid peg (dens). A distance of greater than 6 mm suggests ligamentous injury.
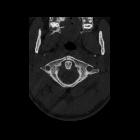
CT
CT demonstrates the fracture line which usually involves both the anterior and posterior arches. If there is an injury to the transverse atlantal ligament, the atlantodental interval (ADI) increases. The normal ADI in the adult population is less than 3 mm; in pediatric populations, the normal distance is less than 5 mm.
MRI
The fracture will not be seen as well as with CT. However, localized soft-tissue injury will be apparent. Pre-vertebral hemorrhage or edema will identify injury at the level of C1/2. A ligamentous injury will also be demonstrated. A fat-sat T2 sequence is useful in the trauma setting to help distinguish abnormal soft-tissue injury from normal fat.
Treatment and prognosis
Jefferson fractures are typically treated conservatively (hard collar immobilization) provided the transverse atlantal ligament is considered intact (no widening of the atlantodental interval or intact ligament visualized on MRI).
In cases where the ligament is thought to be disrupted, the injury is considered unstable and more aggressive management is usually required . This includes halo immobilization, posterior C1-C2 lateral mass internal fixation or transoral internal fixation.
History and etymology
Named by Sir Geoffrey Jefferson (1886-1961), a neurosurgeon from the United Kingdom .
Differential diagnosis
- pseudo-Jefferson fracture, or pseudospread of the atlas on the axis
- refers to the normal overhanging of the lateral edges of the lateral masses of C1 over the lateral edges of the body of C2 seen in children
- split atlas
- rare congenital anatomic anomaly of fusion defects of both the anterior and posterior arches of C1
See also
Siehe auch:
- Frakturen mit Eigennamen
- Frakturen der Wirbelsäule
- Frakturen der Halswirbelsäule
- hangman fracture
- Atlasfrakturen
- Atlas
- Klassifikation Atlasfrakturen nach Gehweiler
und weiter:


 Assoziationen und Differentialdiagnosen zu Jefferson-Fraktur:
Assoziationen und Differentialdiagnosen zu Jefferson-Fraktur: